Premenstrual Dysphoric Disorder Symptoms: Causes, Diagnosis, and Treatment

In my practice as a clinical psychologist, I frequently sit across from high-achieving individuals who feel like they are losing their grip on their identity for two weeks out of every month. They describe a “Jekyll and Hyde” existence where, despite their best efforts, they are overwhelmed by a tide of irritability, despair, and physical pain that seems to vanish the moment their period begins. This is not “bad PMS”; this is Premenstrual Dysphoric Disorder (PMDD) Symptoms
What is PMDD?
Premenstrual dysphoric disorder is a severe, sometimes disabling extension of premenstrual syndrome (PMS). While PMS affects the majority of menstruating individuals with mild bloating or moodiness, PMDD is a clinically recognized health condition affecting approximately 3–8% of the population.
It is characterized by intense emotional, physical, and cognitive symptom burdens that can disrupt careers, strain relationships, and diminish one’s quality of life.
Clinically, PMDD is recognized in the DSM-5 as a depressive disorder and in the ICD-10 as a disease of the genitourinary system. In clinical practice, patients often report mood swings, irritability, and fatigue so severe that daily functioning is disrupted during the luteal phase (the time between ovulation and menstruation).
Because the symptoms are so intense, it is vital to understand that PMDD is a legitimate medical condition, not a character flaw, and it is highly treatable.
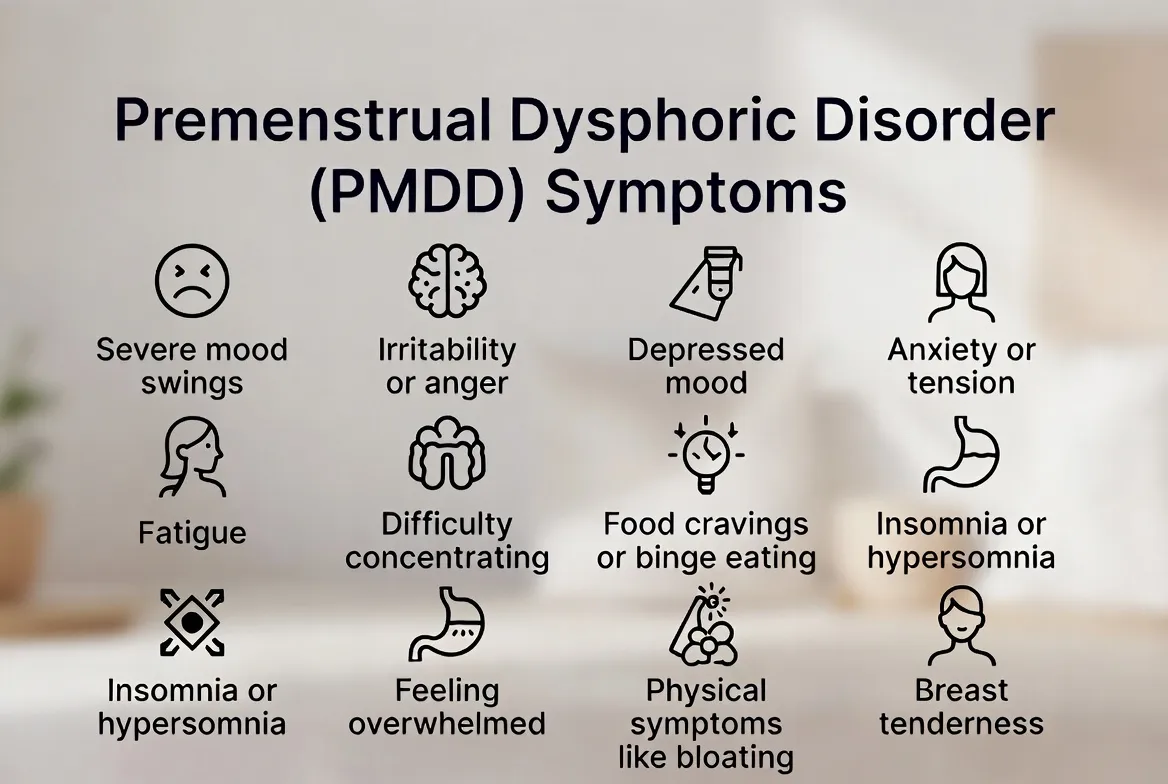
PMDD Symptoms
Understanding premenstrual dysphoric disorder symptoms requires looking beyond the surface level of “feeling moody.” In my practice, I find that patients are often relieved when we break down their experience into three distinct categories: emotional, physical, and cognitive.
For a diagnosis to be made according to premenstrual dysphoric disorder symptoms, DSM-5 criteria, these symptoms must follow a strict cyclical pattern, emerging in the luteal phase and resolving shortly after the period starts.
The Emotional and Cognitive Burden
The psychological impact of PMDD is what differentiates it most sharply from standard PMS. PMDD, premenstrual dysphoric disorder, symptoms often feel like an acute depressive episode that restarts every month.
- Affective Lability (Mood Swings): Feeling suddenly sad or tearful, or increased sensitivity to rejection.
- Marked Irritability or Anger: Increased interpersonal conflicts; feeling “on a short fuse.”
- Depressed Mood: Feelings of hopelessness or self-deprecating thoughts.
- Marked Anxiety: Feeling keyed up or on edge.
- Cognitive “Brain Fog”: This is a failure of executive function. Patients describe an inability to focus on screens, forgetfulness, and a sense of being “disconnected” from their work.
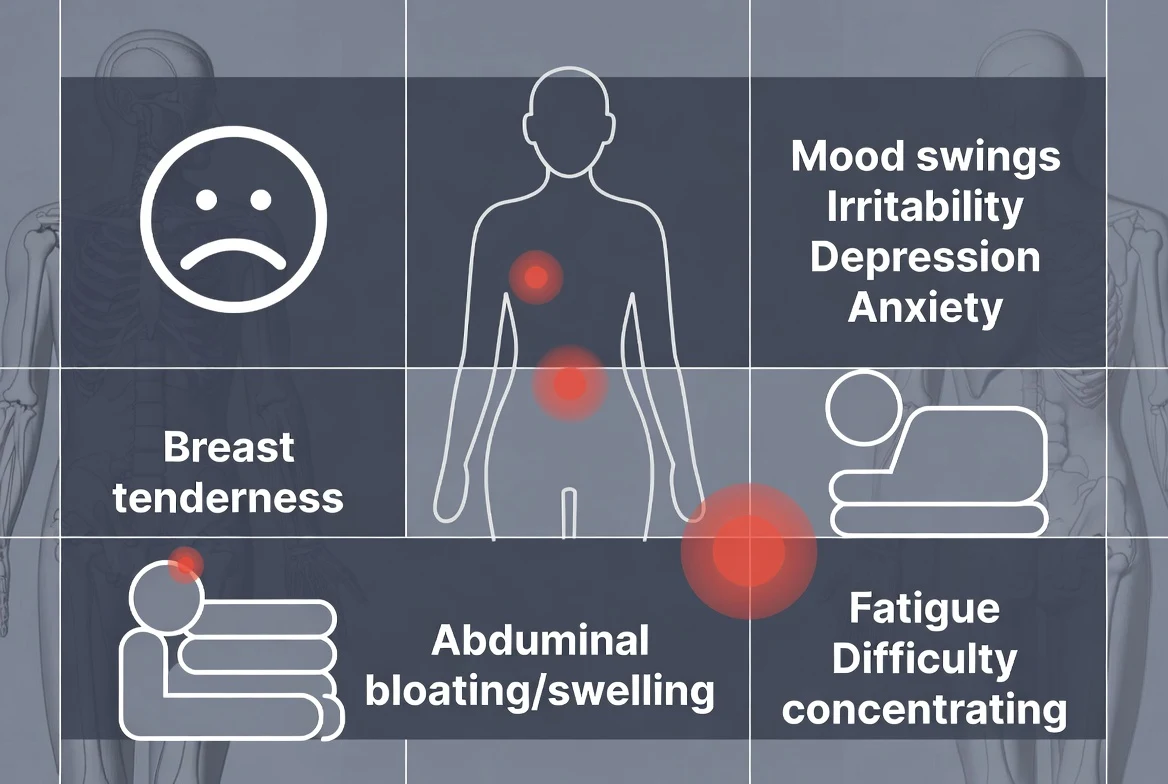
PMDD Physical Symptoms
While the emotional toll is high, the body also pays a price. PMDD physical symptoms are often what first lead patients to seek medical advice:
- Lethargy and Fatigue: A heavy, “leaden” feeling in the limbs that sleep does not fix.
- Physical Sensitivities: Breast tenderness, joint or muscle pain, and headaches.
- Autonomic Changes: Bloating, weight gain, and changes in appetite (specifically cravings for carbohydrates or salty foods).
The Distinction: PMDD Symptoms vs. PMS
The difference between premenstrual dysphoric disorder symptoms and PMS is the degree of functional impairment. While premenstrual dysphoric disorder symptoms, as listed by the NHS and other health organizations, are similar to those of both, PMDD is defined by its ability to stop you in your tracks.
If you are missing work, experiencing suicidal ideation, or having explosive arguments that threaten your marriage only during the week before your period, you are likely dealing with PMDD.
A nuance that only a practicing psychologist might notice is how circadian rhythms and sleep hygiene interact with the luteal phase to worsen symptoms.
The Insight: During the luteal phase, the body’s core temperature rises, which can fragment sleep and reduce REM quality. I once worked with a patient, “Sarah,” who found that her PMDD-related “rage” was nearly uncontrollable on Tuesday mornings.
By looking at her symptom tracker, we noticed her sleep hygiene was poorest on Sunday and Monday nights due to work stress. The lack of sleep combined with the hormonal shift essentially “turned off” her prefrontal cortex.
By stabilizing her sleep environment—lowering the room temperature and using a weighted blanket during those specific ten days—we were able to reduce her irritability by 40% before we even discussed medication.
Causes and Risk Factors
A question I am frequently asked is, “What causes PMDD? “Many assume they have a ‘hormone imbalance.’” However, clinical research suggests that most individuals with PMDD actually have normal hormone levels. The issue isn’t the amount of hormones, but how the brain responds to them.
The Serotonin-Progesterone Link
The leading theory behind premenstrual dysphoric disorder symptoms’ causes is a cellular hypersensitivity to the fluctuations of estrogen and progesterone. When these hormones shift during the luteal phase, they interact with neurotransmitters, specifically serotonin.
In those with PMDD, this hormonal “drop” triggers a corresponding drop in serotonin activity. Since serotonin regulates mood and pain, this creates a neurochemical “crash” every month.
Comorbidities: PMDD and ADHD
In my practice, I see a significant overlap between PMDD and ADHD. Because estrogen helps facilitate dopamine signaling, the drop in estrogen during the luteal phase can make ADHD symptoms feel much worse. Patients often find their ADHD medication “stops working” during this time, leading to extreme emotional lability.
Diagnosis of Premenstrual Dysphoric Disorder
Establishing a premenstrual dysphoric disorder diagnosis is a process of exclusion and data collection. Many patients are initially misdiagnosed with depression or anxiety because they seek help while in the midst of a flare-up.
DSM-5 Criteria
To meet the PMDD DSM-5 standards, a patient must demonstrate the following:
- At least five symptoms are present in the final week before menses.
- At least one symptom must be a mood symptom (irritability, anxiety, or depression).
- Symptoms must improve within a few days after menses begins and become minimal/absent in the week post-menses.
- This pattern must be confirmed by prospective daily tracking for at least two consecutive cycles.
The Importance of Tracking
How is PMDD diagnosed? It is not diagnosed via a blood test. It is diagnosed through the “evidence” of your daily life. I recommend patients use symptom-tracking apps or a paper diary. We look for the “clear week”—a week where the patient feels like their “normal” self.
If there is no clear week of symptom relief, we may be looking at PME (premenstrual exacerbation) of an underlying mood disorder rather than pure PMDD.
Treatment Options
The most encouraging news for my patients is that premenstrual dysphoric disorder treatment is highly effective. We typically use a multi-pronged approach to address both the biological triggers and the psychological fallout.
First-Line Treatment: SSRIs
The best treatment for PMDD often involves Selective Serotonin Reuptake Inhibitors (SSRIs). Interestingly, while SSRIs take weeks to work for clinical depression, they often work within hours or days for PMDD.
Dosing Strategies: Some patients take medication daily, while others use luteal-phase dosing (taking the pill only from ovulation to the start of their period). This targeted approach can minimize side effects like weight gain or sexual dysfunction.
Hormonal Therapy and CBT
Treatment for PMDD also includes hormonal interventions, such as combined oral contraceptives that suppress ovulation, or GnRH agonists for severe cases.
Additionally, Cognitive Behavioral Therapy (CBT) is invaluable. CBT helps patients develop “internal scaffolding”—strategies to manage the intrusive thoughts and irritability so they don’t cause permanent damage to their lives during the two-week flare-up.
Medication Details
When we delve into premenstrual dysphoric disorder symptoms and medication, we are looking at a unique pharmacological landscape. Unlike standard Major Depressive Disorder, where we wait 4–6 weeks for a clinical response, the
“Serotonergic” response in PMDD is remarkably rapid. This is because we aren’t necessarily treating a permanent chemical deficit, but rather a “sensitivity” to the neurosteroid fluctuations in the brain.
The Role of SSRIs
Selective Serotonin Reuptake Inhibitors (PMDD SSRIs) are the gold standard. In my practice, I find that a lower dose than what is typically used for depression often suffices.
- Fluoxetine (Prozac) and sertraline (Zoloft): These are the most common first-line choices. They can be taken “intermittently” (luteal-phase dosing), which many patients prefer to minimize long-term side effects.
- Side Effect Management: While effective, some patients experience nausea or dry mouth. We mitigate this by adjusting the timing of the dose or the specific agent used.
Anxiolytics and Adjuncts
For those with profound, “rage-like” irritability or panic, a premenstrual dysphoric disorder anxiolytic may be prescribed for as-needed use during the peak flare-up days. Precision is key; the medication for PMDD must be tailored to whether the patient’s primary struggle is “leaden” depression or “keyed-up” anxiety.
Self-Care and Lifestyle Strategies
While medication provides the biological “floor,” premenstrual dysphoric disorder self-care is what allows for true functional recovery. I often tell my patients that the luteal phase is a time for “low-arousal living.”
- Nutrition and Inflammation: Reducing caffeine and salt can significantly lower the severity of PMDD physical symptoms like breast tenderness and bloating.
- PMDD Stress Management: This is the time to utilize “pacing.” If you know your executive function will be compromised next Tuesday, we plan your high-stakes work meetings for your follicular phase (the week after your period).
- Mindfulness and Journaling: By “externalizing” the intrusive thoughts, you can remind yourself, “This is the PMDD talking, not my reality.”
Combining medical therapy with structured self-care significantly reduces symptom severity and improves quality of life.
Special Populations and Considerations
The PMDD onset typically occurs in the late teens to early 20s, but it can be particularly volatile during perimenopause. One of the most critical populations I treat involves the intersection of PMDD and ADHD.
Because estrogen drops during the luteal phase, dopamine—the fuel for the ADHD brain—drops with it. I often hear from patients that their stimulant medication “simply stops working” during the week before their period. This can lead to a devastating “double-drop” in mood and focus.
For these patients, we often coordinate with their prescribing physician to adjust their ADHD regimen or introduce an SSRI specifically for that window to protect their mental clarity.
Frequently Asked Questions
Can PMDD be cured?
While we don’t speak of a “permanent cure” in the way we do for an infection, PMDD is highly manageable. Most patients achieve “functional remission,” where they no longer meet the diagnostic criteria after finding the right treatment.
What does a PMDD episode look like?
A typical episode involves a sudden “switch” in personality—one day you are capable and social, and the next you are overwhelmed by “rage,” despair, and physical exhaustion that feels entirely out of your control.
Is PMDD a mental illness?
Yes, the DSM-5 classifies it as a depressive disorder. This classification is vital because it ensures that patients receive evidence-based care and that insurance covers their PMDD therapies.
How long do symptoms last?
Symptoms typically last between 7 and 14 days, appearing after ovulation and ending within the first day or two of menstruation.
Conclusion
Navigating Premenstrual Dysphoric Disorder (PMDD) is a journey of reclaiming your time. By understanding the biological “Why” behind the symptoms and utilizing a multidisciplinary approach to how to treat PMDD, you can stop the cycle of monthly hijacking.
- Track your cycle: Use data to prove the pattern.
- Prioritize sleep: Protect your brain’s CEO during the luteal phase.
- Seek integrated care: Combine post-traumatic stress disorder treatment techniques (like CBT) with pharmacological support.
Early recognition and professional evaluation are the first steps toward a life where you are the driver, not your hormones.
References & Resources
- International Association for Premenstrual Disorders (IAPMD): iapmd.org
- National Institutes of Health (NIH): Anxiety and PMDD Resources
- American College of Obstetricians and Gynecologists (ACOG): Guideline on PMDD
- Bipolar Lives: Clinical Psychologist Insights

Related Posts






Subscribe to Our Newsletter
Get mental health tips, updates, and resources delivered to your inbox.
MORE from Author
Read More In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure…
In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure…- We all have "up" days and "down" days. Perhaps you feel energized after a promotion or sluggish on a rainy…


 To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,…
To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,… To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…
To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…


Are you looking for a Therapist?
Connect with qualified mental health professionals who understand
bipolar disorder, mood changes, and emotional challenges.
Private • Supportive • Confidential