Obsessive-Compulsive Disorder (OCD) ICD-10 and Codes: Diagnosis, Criteria, and Clinical Guidance

In the complex landscape of mental health care, the bridge between a patient’s lived experience and the formal healthcare system is built upon a foundation of standardized language. For those living with Obsessive-Compulsive Disorder (OCD), ICD-10, this language is crystallized in the ICD-10 F42 obsessive-compulsive disorder classification.
While patients often come to me describing a “prison of the mind” or a “broken record of intrusive thoughts,” the medical community requires a more clinical taxonomy to ensure that these individuals receive the life-altering care they deserve.
Assigning the correct obsessive-compulsive disorder ICD-10 code is not merely a bureaucratic exercise. In my clinical practice, I have seen how accurate coding is the gatekeeper to treatment.
It dictates whether an insurance company will authorize specialized exposure and response prevention (ERP) therapy or cover the high-dose SSRIs often required for symptom management. Furthermore, these codes allow us to track global health trends and ensure that researchers are looking at the same clinical populations.
Whether you are a clinician, a medical coder, or an individual seeking to understand your diagnosis, mastering the F42 coding structure is a vital step in navigating the path to wellness.
Understanding OCD in ICD-10
The obsessive-compulsive disorder ICD-10-CM (Clinical Modification) system is designed to provide more than just a general label; it offers a nuanced breakdown of how the disorder manifests in an individual. In my practice, I frequently observe that no two cases of OCD are identical.
One patient may spend six hours a day trapped in mental “loops” (obsessions) with no visible rituals, while another may be compelled to wash their hands until the skin is raw (compulsions) without a clearly articulable fear.
To capture this clinical variety, the obsessive-compulsive disorder ICD-10 structure is broken down into specific subcodes:
The F42 Coding Hierarchy
- F42.0 – Predominantly obsessions (obsessional thoughts or rumination): This code is used when the patient’s distress is primarily driven by intrusive, unwanted ideas, images, or impulses. These often center on “taboo” topics, harm, or existential doubt.
- F42.1 – Predominantly compulsions (obsessional acts): This is assigned when the most prominent feature is repetitive, ritualistic behavior—such as checking, cleaning, or ordering—intended to neutralize a sense of “wrongness” or prevent a catastrophe.
- F42.2 – Mixed obsessions and compulsions: This is the most common presentation I see. Most patients experience a distressing thought (the obsession) that triggers a physical or mental ritual (the compulsion) to alleviate that distress.
- F42.8 – Other OCD: Reserved for presentations that don’t neatly fit the above categories but still meet the core obsessive-compulsive disorder ICD-10 criteria.
- F42.9 – Obsessive-compulsive disorder, unspecified (ICD-10): This acts as a placeholder when a diagnosis of OCD is clear, but the clinician has not yet determined which symptom set is predominant.
The “Why” Behind the Taxonomy
The psychological “why” behind this detailed coding relates to the biological mechanism of the disorder. OCD is essentially a “stutter” in the brain’s cortico-striatal-thalamo-cortical (CSTC) loop.
This circuit is responsible for checking for threats and then “shifting gears” once a threat is resolved. In a patient coded with F42.1, the “motor” part of this loop is stuck on repeat. In a patient with F42.0, the “evaluative” part of the brain is over-firing.
By differentiating these in the medical record, we can better predict treatment response. For instance, someone with predominantly mental obsessions may require a different cognitive “reframing” approach within ERP than someone with overt physical rituals.
Accurate coding also prevents the common error of misdiagnosing OCD as a mood disorder or a generic anxiety condition, ensuring the patient isn’t treated with ineffective “talk therapy” that might actually exacerbate their symptoms.
I once treated a patient, “Mark,” who was initially referred for general anxiety (F41.1). However, upon a deeper dive into his executive function, I realized his “worry” wasn’t about life stressors but a desperate need for absolute certainty regarding a single intrusive thought.
The Nuance: Mark’s response to treatment was heavily influenced by his circadian rhythms. When he was sleep-deprived, his ability to “label” his thoughts as OCD symptoms (a process requiring high-level prefrontal cortex function) plummeted, and his rituals spiked.
By correcting his diagnosis to F42.2 and addressing his sleep hygiene, we moved from “managing stress” to “treating a neurobiological loop.” This change in code changed his entire treatment trajectory.
DSM-5 vs. ICD-10 Criteria
While the obsessive-compulsive disorder DSM-5 is the “gold standard” for clinical diagnosis in the United States, the obsessive-compulsive disorder ICD-10 criteria are the global standard for reporting and billing. Understanding the overlap is essential for any modern healthcare provider.
The DSM-5 criteria focus heavily on the psychological impact: the presence of obsessions or compulsions must be time-consuming (more than one hour per day) and cause significant distress or functional impairment.
The ICD-10 follows a similar path but emphasizes the “unpleasantness” and “ego-dystonic” nature of the symptoms—the fact that the patient recognizes these thoughts as their own yet finds them senseless and impossible to resist.
In my practice, I often use the DSM-5 to conduct a deep-dive diagnostic interview and then “translate” those findings into an ICD-10 code for the patient’s Electronic Medical Record (EMR). This dual literacy ensures that the clinical richness of the patient’s experience is preserved even while adhering to the rigorous requirements of health insurance coding.
Common ICD-10 Codes for OCD and Related Disorders
To assist clinicians and patients in identifying the correct obsessive-compulsive ICD-10 code, I’ve outlined the primary classifications used in a modern psychiatric setting. Choosing the right subcode is often the difference between a claim being approved or denied.
Primary OCD Coding Table
| ICD-10 Code | Clinical Description | Typical Presentation Example |
|---|---|---|
| F42.0 | Predominantly obsessions | Constant “what-if” thoughts about harm without physical rituals. |
| F42.1 | Predominantly compulsions | Hand-washing or door-checking rituals take 3+ hours daily. |
| F42.2 | Mixed obsessions and compulsions | Fear of germs (obsession) followed by disinfecting (compulsion). |
| F42.8 | Other specified OCD | Atypical presentations, such as “Just Right” OCD or scrupulosity. |
| F42.9 | Unspecified OCD | The patient clearly has OCD, but subtypes are not yet clarified. |
In ambiguous cases, I recommend starting with F42.9 while the diagnostic picture matures. However, for the purposes of securing insurance for high-intensity treatments like PHP (Partial Hospitalization) or IOP (Intensive Outpatient) programs, moving to a more specific code like F42.2 is often necessary to demonstrate the complexity of the case.
Other Obsessive-Compulsive Disorders in ICD-10
It is clinically imperative to distinguish primary OCD from other conditions that may mimic obsessive-compulsive behavior in the ICD-10. One of the most frequent diagnostic overlaps I encounter involves Obsessive-Compulsive Personality Disorder (OCPD), which is coded as F60. 5.
While the names are nearly identical, the psychological “why” is worlds apart. OCD is characterized by intrusive thoughts that the patient finds repulsive (ego-dystonic). In contrast, OCPD is a personality style defined by rigidity, perfectionism, and a need for control that the person often views as “correct” or “beneficial” (ego-syntonic). Furthermore, we must distinguish OCD from the following:
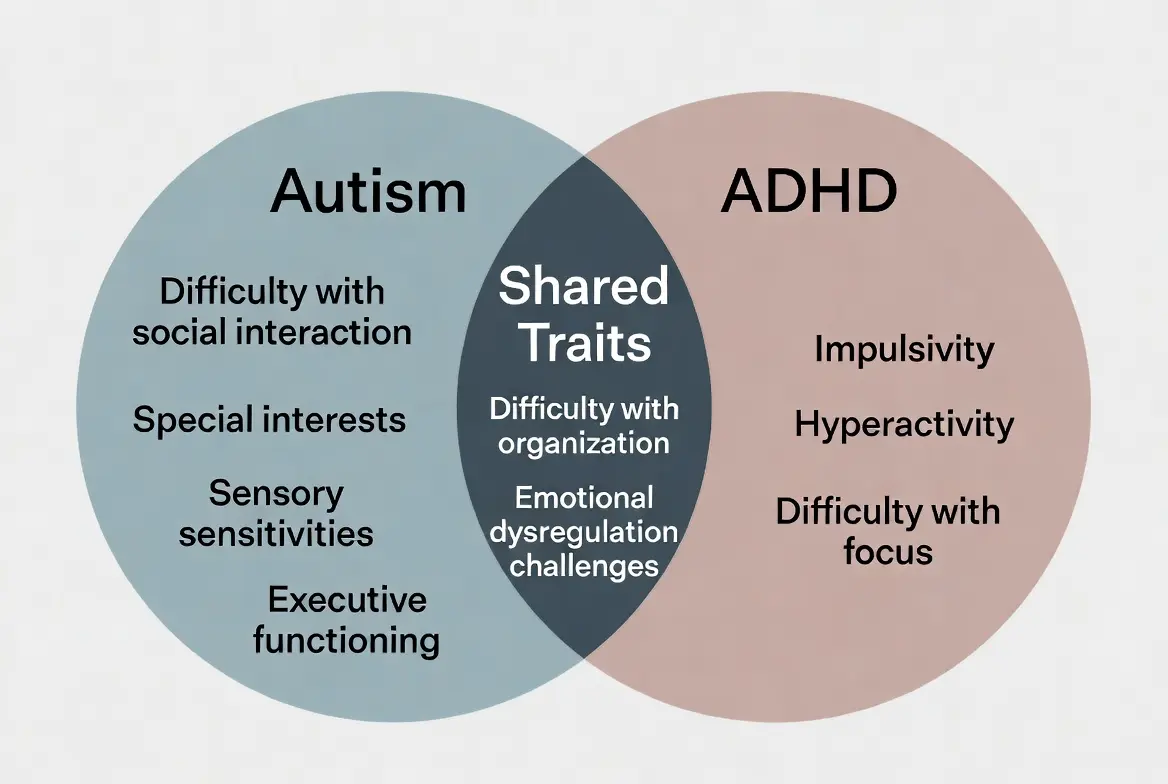
- F90 or F84 codes: Repetitive behaviors in ADHD or autism spectrum disorders, where the behavior is often a “stim” or a regulatory tool rather than a response to a distressing obsession.
- F42.8: This code includes “other” specified disorders, such as body dysmorphic disorder or hoarding disorder, which share the OCD “loop” but focus on specific themes like physical appearance or the acquisition of objects.
In my practice, I have found that misclassifying OCPD as OCD can lead to months of ineffective treatment; OCPD typically requires a focus on interpersonal dynamics and flexibility, whereas OCD requires the behavioral “challenge” of ERP.
OCD Symptoms and Clinical Presentation
The obsessive-compulsive disorder symptoms in DSM-5 and ICD-10 are largely aligned, focusing on the pervasive nature of the “loop.” When I am assessing a patient for an F42 diagnosis, I look for three specific markers:
- Obsessions: These are not just “worries.” They are intrusive, often terrifying images or impulses that feel like they have “hijacked” the mind.
- Compulsions: These are the “safety behaviors.” They can be overt (checking a lock) or covert (mentally reviewing a conversation to ensure nothing offensive was said).
- Avoidance: This is the invisible symptom. To avoid the terror of an obsession, a patient might stop driving, stop using public restrooms, or withdraw from social life entirely.
In children, these symptoms often present as “magical thinking”—believing that jumping over a crack in the sidewalk will protect a parent from illness. In adults, the symptoms are often more complex and shrouded in shame, particularly when they involve “taboo” intrusive thoughts.
ICD-10 Coding in Clinical Practice
For the clinician or medical coder, selecting the right obsessive-compulsive disorder ICD-10 CM code is a step-by-step process of elimination:
- Establish the Diagnosis: Does the patient spend more than one hour per day on these thoughts/acts? Is it causing functional impairment?
- Determine Predominance: If the patient says, “I have the thoughts, but I don’t really do anything about them,” look toward F42.0. If they say, “I just have to wash my hands until they feel right, I’m not even sure why,” F42.1 is more appropriate.
- Document Severity: For insurance purposes, it isn’t enough to list the code. You must document the Y-BOCS score or the specific ways the disorder prevents the patient from working or attending school.
Accurate coding reduces the “administrative friction” between the patient and their care. It ensures that when I prescribe a high-dose SSRI, the pharmacist and the insurance provider understand that this is for a chronic neurobiological condition (OCD) rather than a temporary depressive episode.
OCD Treatments and ICD-10 Relevance
The obsessive–compulsive disorder treatments we select are directly linked to the code on the chart. Most health insurance plans have specific “medical necessity” guidelines for OCD:
- Pharmacotherapy: To approve high-dose SSRIs (sertraline, fluoxetine) or clomipramine, insurers look for the F42 code.
- Behavioral Therapy: ERP is a highly specialized, often more expensive form of therapy. Correct coding ensures that the therapist is reimbursed for the specific technical labor required to treat the CSTC loop.
- Intensive Treatment: If a patient requires residential or intensive outpatient care, the ICD-10 code provides the statistical “weight” needed to justify that level of intervention.
Frequently Asked Questions
What is the ICD-10 code for OCD?
The primary code is F42, which is then subdivided based on whether the patient has predominantly obsessions, compulsions, or a mixture of both.
What is the difference between F42.8 and F42.9?
F42.8 is used for “Other specified” OCD (where the presentation is unique but known), while F42.9 is “Unspecified,” used when the diagnosis is certain but the specific subtype hasn’t been determined yet.
Is OCPD included in the OCD ICD-10 codes?
No. Obsessive-Compulsive Personality Disorder is a separate clinical entity and is coded under personality disorders as F60. 5.
Conclusion
Mastering the obsessive-compulsive disorder ICD-10 framework is an act of clinical advocacy. By ensuring that every patient is coded accurately—whether as F42.0, F42.1, or F42.2—we ensure they have access to the evidence-based treatments that can break the “loop” of OCD.
The transition from a “doubting disease” to a life of certainty begins with an accurate diagnosis. If you or a loved one is struggling with these symptoms, remember that a formal code is not a life sentence; it is a roadmap to the right help.
References & Resources
- World Health Organization (WHO): ICD-10 Browser – F42 OCD
- American Psychiatric Association: DSM-5-TR Fact Sheets
- International OCD Foundation (IOCDF): Clinical Guidance and Specialist Finder
- Bipolar Lives: Expert Psychologist Resources

Related Posts



Subscribe to Our Newsletter
Get mental health tips, updates, and resources delivered to your inbox.
MORE from Author
Read More In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure…
In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure…- We all have "up" days and "down" days. Perhaps you feel energized after a promotion or sluggish on a rainy…


 To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,…
To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,… To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…
To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…


Are you looking for a Therapist?
Connect with qualified mental health professionals who understand
bipolar disorder, mood changes, and emotional challenges.
Private • Supportive • Confidential