Post-Traumatic Stress Disorder (PTSD) Symptoms: Causes, Types, and Treatments
In my practice as a clinical psychologist, I often sit across from individuals who feel as though they are living in two timelines at once. They are physically present in my office, yet a part of their nervous system is permanently anchored to a moment of past trauma. This is the hallmark of Post-Traumatic Stress Disorder (PTSD) Symptoms—a condition where the brain’s “alarm system” fails to return to baseline after a threat has passed.
The post-traumatic stress disorder definition has evolved significantly over the years. According to the DSM-5-TR, PTSD is a trauma- and stressor-related disorder that develops following exposure to an event involving actual or threatened death, serious injury, or sexual violence.
Clinically, PTSD manifests differently across patients—some experience vivid flashbacks, while others report persistent hypervigilance or emotional numbing. We also now recognize complex PTSD (C-PTSD), which arises from prolonged, repeated trauma rather than a single event.
Early recognition of post-traumatic stress disorder symptoms is key to improving daily functioning. When we identify these patterns early, we can utilize the brain’s inherent neuroplasticity to “rewire” the trauma response before it becomes a deeply ingrained “worry groove.”
This article explores the nuanced symptoms, underlying causes, and evidence-based treatments that allow patients to move from a state of survival back into a state of living.
Understanding PTSD Symptoms
To understand why PTSD symptoms feel so pervasive, we must look at the “why” behind the biology. In a neurotypical brain, a traumatic memory is processed by the hippocampus and “filed away” as a past event.
In an individual with PTSD, the memory remains “hot” and is stored in the amygdala—the brain’s fear center. This creates a state where the body reacts to a memory as if it were a current, life-threatening reality.
The DSM-5 categorizes post-traumatic stress disorder symptoms into four primary clusters, each representing a different way the nervous system attempts to manage the “stuck” trauma.
A. Intrusion Symptoms
These are the most well-known signs of post-traumatic stress disorder. They include involuntary, distressing memories, nightmares, and flashbacks.
- The Biology: When the amygdala is hyper-responsive, it bypasses the logical prefrontal cortex. A simple sensory trigger—like the scent of a certain cologne or the sound of a car backfiring—signals a “Code Red.” The brain initiates a full sympathetic nervous system response, causing the person to physically and emotionally “relive” the trauma.
B. Avoidance Behaviors
Patients go to great lengths to avoid people, places, or even internal thoughts that remind them of the event.
- Psychology: Avoidance is a primary defense mechanism. However, it creates a “feedback loop” of fear. By avoiding the trigger, the brain never learns that the current environment is safe. This reinforces the trauma’s power over the individual’s life.
C. Negative Alterations in Cognition and Mood
This cluster includes persistent negative beliefs about oneself (“I am bad,” “The world is dangerous”) and emotional numbing. Many patients report a loss of interest in activities they once loved.
- The Biology: Chronic trauma can lead to a “shutdown” state. When the brain is in constant fight-or-flight, it de-prioritizes the “social engagement system.” This often results in a feeling of being “spaced out” or disconnected from loved ones.
D. Hyperarousal and Reactivity
This involves being easily startled, feeling “on edge,” irritability, and significant sleep disturbances.
- The Biology: This is a state of permanent hypervigilance. The brain’s executive function is depleted because all energy is being funneled into scanning the environment for threats. This leads to profound physical symptoms of PTSD, such as chronic muscle tension, fatigue, and headaches.
| Symptom Cluster | Common Manifestations | Clinical Impact |
| Intrusion | Flashbacks, Nightmares | High acute distress |
| Avoidance | Staying home, suppressing memories | Social/Occupational isolation |
| Cognition/Mood | Shame, memory gaps, numbing | Loss of identity |
| Hyperarousal | Startle response, anger, insomnia | Physical exhaustion |
Complex PTSD Symptoms
In practice, patients with complex post-traumatic stress disorder symptoms often struggle with interpersonal relationships and identity issues that go beyond the standard PTSD diagnosis. C-PTSD typically results from “Type II” trauma—prolonged exposure to trauma from which escape is difficult, such as childhood neglect or long-term domestic captivity.
In addition to the standard clusters, C-PTSD involves “Disturbances in Self-Organization” (DSO). Patients often experience profound emotional dysregulation, a persistent sense of worthlessness, and a chronic inability to trust others.
I often observe that these patients don’t just feel they have a problem; they feel they are the problem. Their executive function is often compromised not just by fear, but by a fragmented sense of self.
Causes and Risk Factors
Why do some individuals experience a traumatic event and recover, while others develop post-traumatic stress disorder symptoms? The post-traumatic stress disorder causes are a “perfect storm” of biological and environmental factors.
- Traumatic Triggers: Combat, sexual assault, natural disasters, and serious accidents are common catalysts.
- Biological Vulnerability: Some individuals are born with a more sensitive HPA axis. (the body’s stress response system), making them more prone to “getting stuck” in a stress loop.
- Early Life Trauma: Childhood trauma can “prime” the nervous system, making it more reactive to stressors later in life.
- Social Support: A lack of immediate support following a trauma is a significant risk factor for the development of chronic PTSD.
Conversely, some patients experience post-traumatic growth. With the right support, the process of navigating trauma can lead to increased personal strength and a revised appreciation for life.
Symptom Variations Across Populations
Recognizing physical and subtle emotional symptoms is critical—many patients initially present with somatic complaints rather than psychological distress.
Signs of PTSD in Men vs. Women
Symptoms of PTSD in women often lean toward internalizing behaviors, such as depression, anxiety, and self-blame. Women are also statistically more likely to experience intrusive memories and emotional numbing.
In contrast, signs of PTSD in men often manifest as “externalizing” behaviors. This may include increased irritability, anger outbursts, or substance use as a form of self-medication.
“Weird” and Physical Symptoms
I often hear patients describe “weird” symptoms of PTSD, such as
- Somatic Complaints: Unexplained gastrointestinal issues, heart palpitations, or chronic pain.
- Dissociation: Feeling like the world is “unreal” or like they are watching their life from outside their body.
- Emotional Numbing: An inability to feel joy, even during major life milestones.
Clinical Insight: The Sleep-Hygiene Connection
A nuance that many overlook is how a patient’s circadian rhythms dictate their ability to process trauma.
The Insight: I once worked with a patient, “Mark,” who was making little progress in EMDR therapy. We discovered his sleep was fragmented by night terrors, leading him to rely on caffeine throughout the day. This “tired-wired” state kept his amygdala in a state of high arousal. By implementing strict sleep
hygiene—stabilizing his internal clock before diving back into trauma work—his prefrontal cortex finally had the “fuel” needed to regulate his emotions. Without sleep, the brain cannot facilitate the neuroplasticity required for healing.
Comprehensive Symptom Lists
In my practice, I find that providing patients with a post-traumatic stress disorder symptoms list is often the first step toward reducing their shame. When symptoms are labeled, they move from being “personal failings” to recognized clinical markers. Depending on the diagnostic framework used (DSM-5 vs. ICD-11), the number of recognized symptoms can vary.
The 5 Core Symptoms of PTSD
Most clinicians look for these primary indicators during a baseline screening:
- Re-experiencing: Flashbacks or vivid nightmares.
- Avoidance: Steering clear of people or places that trigger memories.
- Hypervigilance: A constant sense of “scanning” for danger.
- Emotional Numbing: Feeling detached or unable to experience “warm” emotions.
- Exaggerated Startle Response: Jumping at loud noises or unexpected movements.
The Extended 17–20 Symptom Profile
For a formal diagnosis, we look at a more comprehensive list of 17 to 20 symptoms that span cognitive, physical, and behavioral domains:
- Cognitive/Mood: Inability to remember key aspects of the trauma, persistent distorted blame of self or others, and an “estrangement” from social circles.
- Physical: Chronic fatigue, tension headaches, and gastrointestinal distress caused by a hyperactive sympathetic nervous system.
- Behavioral: Reckless or self-destructive behavior, irritability that manifests as verbal or physical aggression, and profound difficulty concentrating.
Diagnosis and Screening

Establishing a formal diagnosis requires more than just checking boxes on a list. As a psychologist, I must determine if the post-traumatic stress disorder criteria meet the threshold of functional impairment for at least one month.
We utilize several standardized “Gold Standard” tools:
- PCL-5: A 20-item self-report measure that tracks the severity of symptoms over the past month.
- CAPS-5: The Clinician-Administered PTSD Scale, which is the benchmark for determining a definitive diagnosis.
A major part of my role is differential diagnosis. I must ensure that what looks like PTSD isn’t actually bipolar disorder (due to irritability), a traumatic brain injury (TBI), or generalized anxiety disorder. This is where a clinical interview becomes irreplaceable; we look for the “Trauma Nexus”—the specific link between a traumatic event and the subsequent symptoms.
Impact on Daily Life
How does PTSD affect a person’s daily life? In reality, it is a thief of time and energy. When your brain is stuck in “survival mode,” your executive function—the part of the brain that helps you plan, organize, and manage time—is constantly “offline.”
- Work Performance: Many patients struggle with “brain fog” or an inability to focus on complex tasks because their brain is prioritizing threat detection over productivity.
- Social Withdrawal: To avoid triggers, patients often shrink their social worlds. This leads to a secondary “depression of isolation,” which can be as debilitating as the PTSD itself.
- Physical Health: Living in a state of chronic high cortisol leads to “allostatic load”—the physical wear and tear on the heart and immune system.
Evidence-Based PTSD Treatments
The most encouraging news I can give my patients is that the brain is capable of change. Post-traumatic stress disorder treatments have advanced significantly, moving away from simple “talk therapy” toward interventions that target the nervous system directly.
Specialized Psychotherapy
- Cognitive Behavioral Therapy (CBT): We work on identifying “stuck points”—the lies the trauma tells you, such as “It was my fault” or “Nowhere is safe.”
- Exposure Therapy: By safely and gradually approaching trauma-related memories, we promote neuroplasticity, teaching the amygdala that the “memory” is not a “current threat.”
- EMDR (Eye Movement Desensitization and Reprocessing): This uses bilateral stimulation to help the brain move a “stuck” memory from the amygdala into the hippocampus, where it can be filed away as a past event.
Pharmacotherapy
While medication doesn’t “cure” trauma, it can provide a biological “floor.” SSRIs (sertraline, paroxetine) are the only FDA-approved medications for PTSD, helping to stabilize mood and reduce the baseline of anxiety. For those struggling with trauma-induced nightmares, medications like Prazosin can be life-changing by blocking the adrenaline spikes that occur during sleep.
Frequently Asked Questions
Can PTSD go away on its own?
While some people experience “natural recovery” in the first few weeks following a trauma, true PTSD rarely disappears without intervention. Left untreated, it often becomes a chronic condition that “hardens” into the personality.
How do triggers affect symptom intensity?
Triggers act as a “shortcut” to the amygdala. Even if you are having a “good day,” a specific trigger can cause an immediate 1-to-100 spike in anxiety. Therapy helps increase the “gap” between the trigger and your reaction.
What is the most common misdiagnosis?
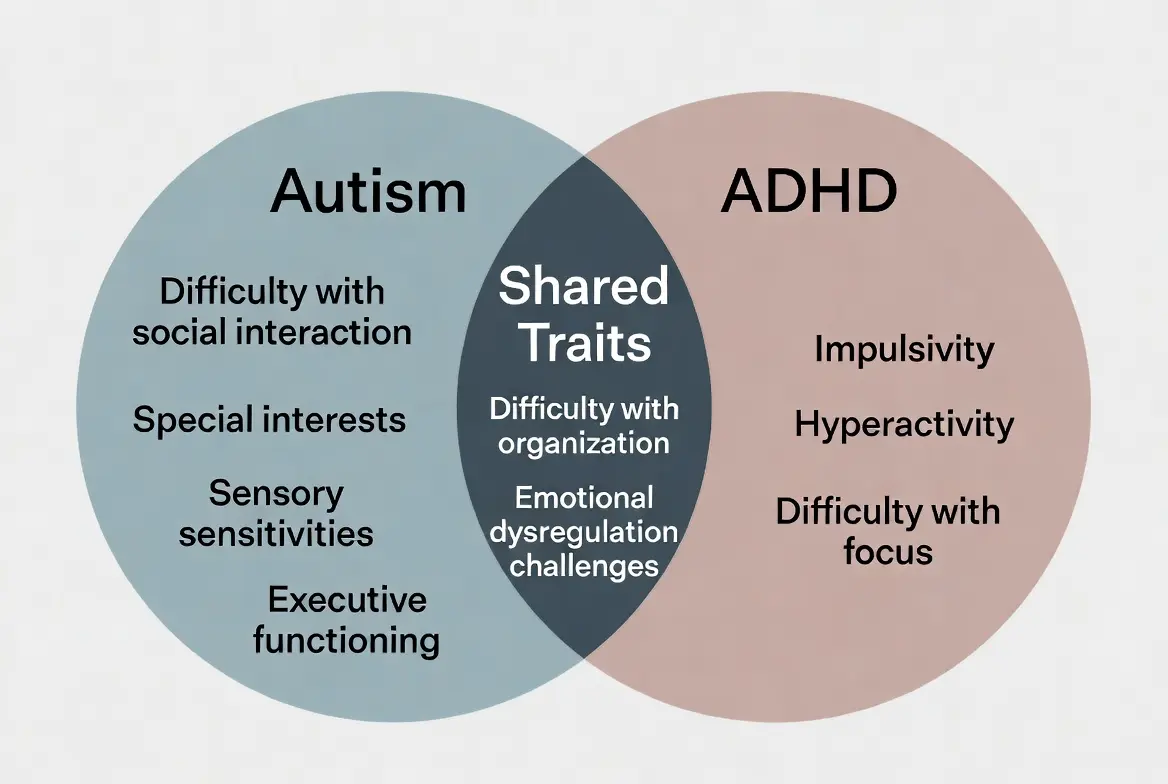
PTSD is frequently misdiagnosed as Borderline Personality Disorder (due to emotional dysregulation) or ADHD (due to concentration issues). A trauma-informed evaluation is essential for an accurate diagnosis.
Conclusion
Navigating post-traumatic stress disorder is an exhausting journey, but it is one that has a map. By understanding the four symptom clusters—intrusion, avoidance, mood changes, and hyperarousal—you can begin to externalize the disorder. It is not “who you are”; it is a set of symptoms resulting from a biological “glitch” in how your brain processed a terrible event.
With integrated care—combining CBT, EMDR, or medication—you can reclaim your identity and your future. If you recognize these signs in yourself, I encourage you to seek a professional consultation. The goal is not just to “cope,” but to thrive.
References & Resources
- National Institute of Mental Health (NIMH): PTSD Overview
- U.S. Dept. of Veterans Affairs: National Center for PTSD
- International OCD Foundation (IOCDF): Trauma and OCD Overlap
- Bipolar Lives: Expert Author Profiles

Related Posts



Subscribe to Our Newsletter
Get mental health tips, updates, and resources delivered to your inbox.
MORE from Author
Read More In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure…
In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure…- We all have "up" days and "down" days. Perhaps you feel energized after a promotion or sluggish on a rainy…


 To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,…
To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,… To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…
To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…


Are you looking for a Therapist?
Connect with qualified mental health professionals who understand
bipolar disorder, mood changes, and emotional challenges.
Private • Supportive • Confidential