Serotonin Reuptake Inhibitors For Anxiety: How They Work, Best Options, Side Effects & What to Expect

Medically reviewed by Laura Athey Updated Date: March 4, 2026
In my practice as a clinical psychologist, I often sit across from individuals whose lives have been narrowed by the relentless static of anxiety. Serotonin reuptake inhibitors for anxiety. They describe a world where “what-ifs” govern their schedule and where the physical sensation of dread—tightness in the chest, shallow breathing, a racing heart—is a constant companion.
When the conversation turns toward pharmacological support, specifically Selective Serotonin Reuptake Inhibitors (SSRIs), I often see a mix of hope and deep-seated hesitation.
I remember a patient I’ll call “Mark,” who struggled with severe Generalized Anxiety Disorder (GAD). Mark was a high-functioning architect, but his internal world was a blueprint of catastrophes.
He was hesitant to try serotonin reuptake inhibitors for anxiety because he feared losing his “creative edge” or feeling “chemically lobotomized.” We spent several sessions discussing the selective serotonin reuptake inhibitors’ definition and how these medications actually interface with the brain’s biology.
What Mark eventually discovered—and what I emphasize to all my patients—is that SSRIs are not “happy pills” designed to manufacture false euphoria. Rather, they are tools that can lower the “volume” of the amygdala’s alarm system, providing the cognitive space necessary for therapeutic work like neuroplasticity and behavioral change to finally take hold.
What Are Selective Serotonin Reuptake Inhibitors (SSRIs)?
To understand why these medications are the frontline defense against anxiety, we must first define the acronym. SSRI stands for Selective Serotonin Reuptake Inhibitor. These are a class of antidepressants that, despite their name, are now considered the “gold standard” for treating various anxiety disorders.
Selective serotonin reuptake inhibitors (SSRIs) are drugs commonly prescribed for the following:
- Generalized Anxiety Disorder (GAD)
- Panic Disorder
- Social Anxiety Disorder
- Obsessive-Compulsive Disorder (OCD)
- Post-Traumatic Stress Disorder (PTSD)
While they all share the same primary mechanism of action, the SSRI drugs list includes several distinct medications, each with its own chemical nuance. Common SSRI medications include:
- Sertraline (Zoloft)
- Escitalopram (Lexapro)
- Fluoxetine (Prozac)
- Paroxetine (Paxil)
- Fluvoxamine (Luvox)
It is important to distinguish these from serotonin-norepinephrine reuptake inhibitors (SNRIs), such as venlafaxine (Effexor) or duloxetine (Cymbalta). While SNRIs also target serotonin, they add a second layer by increasing norepinephrine. In my clinical experience, we often start with an SSRI because they are generally better tolerated and have a simpler side-effect profile for those whose primary symptom is high-arousal anxiety.
How Do SSRIs Work?
When patients ask, “How do selective serotonin reuptake inhibitors work?” I like to use the metaphor of a biological “recycling system.”
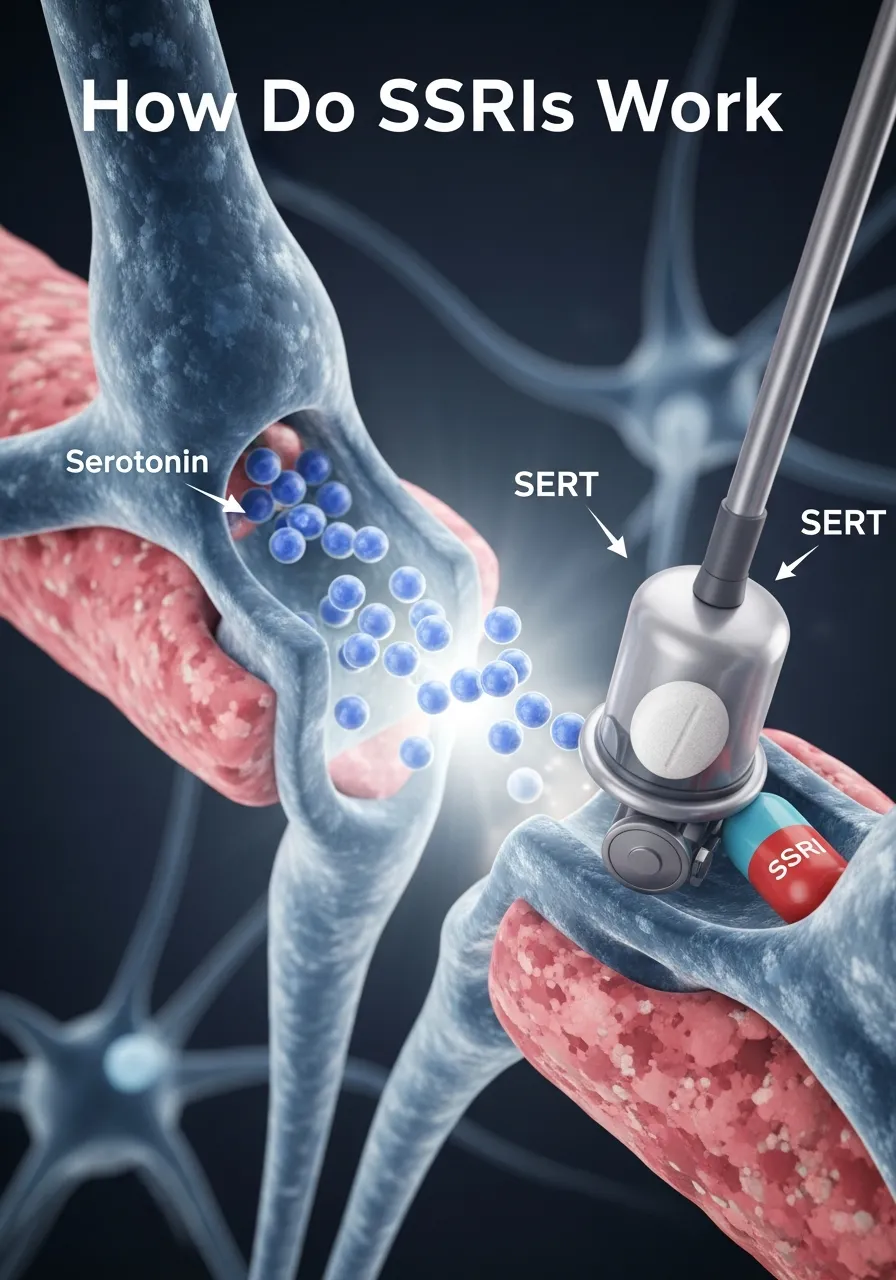
The Synaptic Gap
In your brain, neurons communicate by releasing neurotransmitters like serotonin into a tiny space between them called the synapse. Serotonin is often called the “calming chemical” because it plays a vital role in regulating mood, sleep, and the stress response.
After serotonin delivers its message to the next neuron, the brain naturally “recycles” it through a process called reuptake. A protein called the serotonin transporter (SERT) acts as a vacuum, sucking the serotonin back into the original neuron to be used later.
Blocking the Reuptake
Selective serotonin reuptake inhibitors work by sitting on that “vacuum cleaner.” By blocking the reuptake pump, the medication allows more serotonin to remain in the synaptic gap for a longer period. This increased availability strengthens the communication between neurons, essentially “reinforcing” the brain’s natural ability to regulate anxiety.
The Timeline of Change
A common source of frustration is the delay in relief. Patients often ask, “How long does a serotonin reuptake inhibitor take to work?” If the chemical change happens within hours of the first dose, why don’t you feel better immediately?
The answer lies in neuroplasticity. The initial increase in serotonin triggers a cascade of biological events. Over several weeks, your brain actually begins to desensitize certain stress receptors and increase the production of proteins that repair and grow neural connections. This is a structural shift, not just a chemical one.
| Timeline | What to Expect |
| Week 1–2 | “The Adjustment Phase.” You may feel “jittery” or have mild nausea. Anxiety may temporarily spike. |
| Week 3–6 | “The Turning Point.” Physical symptoms of anxiety (tight chest, racing heart) begin to soften. |
| Week 8–12 | “Full Therapeutic Effect.” This is when we assess if the dose is truly effective for long-term stability. |
Are SSRIs Effective for Anxiety?
From an evidence-based perspective, the answer is a resounding yes. SSRIs are currently categorized as the first-line SSRI for anxiety by major medical bodies, including the American Psychiatric Association.
In my practice, I observe that while they are highly effective, they are most powerful when combined with cognitive behavioral therapy (CBT). The medication handles the “bottom-up” physical arousal, while therapy handles the “top-down” cognitive loops.
Specificity of Treatment
Not all SSRI drugs used for anxiety perform identically across different disorders:
- For panic disorder, we look for medications that are “smooth” and don’t cause too much initial stimulation, like sertraline.
- For OCD, this often requires much higher doses of SSRIs (like fluvoxamine) than what is used for standard depression.
- For GAD: Escitalopram is often favored for its high selectivity and lower rate of drug-to-drug interactions.
The effectiveness of SSRIs for anxiety is well-documented, but the clinical nuance lies in matching the specific drug to the patient’s unique “anxiety thumbprint.”
FDA-Approved SSRIs for Anxiety
While clinicians often prescribe these medications “off-label” based on strong research, it is helpful to know which SSRIs approved for anxiety have gone through the rigorous FDA vetting process for specific indications.
FDA-Approved Indications Table
| SSRI | FDA-Approved Anxiety Indications | Clinical Notes |
| Sertraline | Panic, Social Anxiety, PTSD, OCD | Highly versatile; often the “workhorse” of anxiety treatment. |
| Escitalopram | Generalized Anxiety Disorder (GAD) | Known for being very “clean” with fewer side effects. |
| Paroxetine | GAD, Panic, Social Anxiety, PTSD, OCD | Very effective for physical symptoms, but harder to taper off. |
| Fluoxetine | OCD, Panic Disorder | Long half-life; good for those who might occasionally miss a dose. |
| Fluvoxamine | OCD | Specifically targeted toward obsessive thoughts and compulsions. |
When discussing the best SSRI for extreme anxiety, I tell patients that “best” is a subjective term. What worked for your neighbor might not work for you because your liver metabolism and receptor sensitivity are unique.
Which SSRI Is Best for Anxiety?
In my practice, we don’t pick a medication out of a hat. We use a decision-support framework to determine which SSRI that helps with anxiety is the right fit for your life.
a. The “Side Effect Profile” Priority
If a patient is terrified of weight gain, we might lean toward fluoxetine or escitalopram. If a patient struggles with severe insomnia alongside their anxiety, the more sedating properties of paroxetine might be a “two-birds-one-stone” solution.
b. Comorbid Conditions
Does the patient also have chronic pain? We might consider an SNRI instead. Do they have a history of bipolar disorder? If so, we must be extremely cautious, as SSRIs can sometimes trigger a manic episode if not paired with a mood stabilizer.
c. Genetic Sensitivity
I often observe that patients who have failed multiple medications benefit from pharmacogenomic testing. This looks at how your enzymes break down these drugs. While not a “crystal ball,” it can explain why Mark felt “poisoned” by one SSRI but found immediate relief with another.
A nuance I often discuss with my patients is the “circadian tripwire.” Many people with anxiety have deeply disrupted Circadian Rhythms—they are “night owls” by necessity because that is when the world is quiet. However, SSRIs can be stimulating in the first few weeks.
If a patient has poor sleep hygiene (scrolling on a phone until 2 AM), the initial “jitteriness” of a new SSRI will be amplified tenfold. I have found that patients who commit to a “digital sunset” and consistent wake times during the first 14 days of an SSRI have a 50% lower rate of early discontinuation due to side effects. When we stabilize the clock, we stabilize the response to the medication.
SSRI Side Effects

In my practice, I find that anxiety often feeds on the “fear of the unknown.” Patients like Mark aren’t just worried about the anxiety itself; they are worried about the SSRI side effects they might encounter. It is important to be direct: almost everyone experiences some shift in the first two weeks, but for the majority, these are transient.
Common Early Side Effects
When you first start a medication, your body is adjusting to a systemic increase in serotonin. Since about 95% of your body’s serotonin is actually in your gut, the most common early signs are the following:
- Nausea and GI Upset: This is usually the result of serotonin receptors in the digestive tract being activated.
- Increased “Jitters”: Ironically, SSRI medications can temporarily make you feel more anxious for the first 7–10 days. I often warn patients that they might feel “caffeinated” or restless.
- Headaches and Sleep Changes: You may experience vivid dreams or difficulty falling asleep as your circadian rhythms recalibrate.
Addressing Specific Concerns
Patients often come to me with very specific questions gathered from deep dives into medical forums. Let’s look at the “why” behind some of these:
- Do SSRIs cause weight gain? It depends on the molecule. Paroxetine is the most likely to cause weight changes, while escitalopram and fluoxetine are generally considered weight-neutral. The “why” is often related to changes in insulin sensitivity or a simple return of appetite once the anxiety-induced nausea subsides.
- Can SSRIs cause numbness and tingling? This is a common query. While paresthesia (tingling) can be a side effect, it is often a symptom of the anxiety itself. Hyperventilation—even subtle—changes the CO₂ levels in your blood, leading to tingling in the hands and face.
- Can sertraline cause a rash, or Zoloft cause muscle twitching? While rare, these can occur. A rash should always be reported to your doctor immediately. Muscle twitching (myoclonus) is often a benign sign of increased serotonin activity, but if it is accompanied by a fever, it requires urgent review.
Pros and Cons of SSRIs for Anxiety
Deciding to start an SSRI is a cost-benefit analysis. As a psychologist, my role is to help you weigh these factors against the “cost” of remaining in a state of chronic high-arousal anxiety.
The Benefits (The Pros)
- Emotional “Buffer”: SSRIs provide a floor so your mood doesn’t drop too low and a ceiling so your anxiety doesn’t spiral into panic.
- Non-Addictive: Unlike benzodiazepines (like Xanax), SSRIs do not create a physiological “craving” or a need for ever-increasing doses to achieve the same effect.
- Cognitive Space: By quieting the amygdala, these drugs restore your executive function, allowing you to use the tools you learn in therapy.
The Drawbacks (The Cons)
- Delayed Onset: You have to invest weeks of patience before seeing a “return.”
- Sexual Side Effects: This is the most common long-term reason for discontinuation. Decreased libido or difficulty reaching orgasm can occur.
- Discontinuation Syndrome: You cannot stop these drugs “cold turkey.” Doing so can cause a “brain zap” sensation, dizziness, and a spike in irritability.
SSRIs vs. Serotonin Supplements
A frequent question in our modern “wellness” era is, do serotonin supplements actually improve mood and sleep? Many patients ask if they can take 5-HTP or St. John’s Wort instead of a prescription.
As a clinician, I advise extreme caution here. Supplements lack the selective nature of SSRIs. While an SSRI targets the recycling of serotonin you already have, supplements try to force the production of more.
This is less precise and carries a higher risk of serotonin syndrome—a rare but dangerous “overload” of serotonin—especially if mixed with other medications. Furthermore, the evidence for supplements in treating clinical-grade anxiety disorders is significantly weaker than the robust data we have for SSRIs.
Who Should Not Take SSRIs?
While SSRIs are remarkably safe for the general population, there are specific “red flags” that I screen for in every intake session:
- Undiagnosed Bipolar Disorder: This is perhaps the most critical. If a person has a history of mania (even mild hypomania), an SSRI can act as a “manic switch,” causing a dangerous escalation in energy, spending, and impulsivity.
- MAOI Users: You cannot combine SSRIs with monoamine oxidase inhibitors; the interaction is toxic.
- Pregnancy and Breastfeeding: This is not a “hard no,” but it requires a nuanced conversation with a reproductive psychiatrist to balance the risks of the medication against the risks of untreated maternal anxiety.
What to Expect When Starting: A Practical Guide
If you and your doctor decide to move forward, here is the “road map” I give my patients to ensure success:
- The Low-and-Slow Start: We almost always start at a subtherapeutic dose to “introduce” the drug to your system, then slowly titrate up.
- The “Sidekick” Strategy: Sometimes, I recommend a short-term, as-needed medication to help with the “startup jitters” of the first two weeks.
- The 8-Week Review: Don’t judge the medication on day 10. We wait until the 8-week mark to see if we need to adjust the dose or pivot to a different option.
Frequently Asked Questions
Are SSRIs effective for anxiety?
Yes. They are considered the first-line pharmacological treatment for almost all major anxiety disorders due to their ability to stabilize the brain’s stress response over time.
How long does an SSRI take to work?
While some physical calming may start within 2 weeks, it typically takes 4 to 6 weeks for a significant reduction in anxious thoughts and 8 to 12 weeks for the full therapeutic benefit.
Which SSRI is best for generalized anxiety disorder?
Escitalopram (Lexapro) and sertraline (Zoloft) are often the preferred choices for GAD due to their high efficacy and relatively mild side-effect profiles.
Do SSRIs make you emotionally numb?
This is a common fear. While some people feel “flattened,” this is usually a sign that the dose is too high. The goal is to “trim the peaks” of anxiety, not to remove your ability to feel joy.
What is the most common SSRI for anxiety?
Sertraline (Zoloft) is the most widely prescribed SSRI for anxiety worldwide, largely due to its extensive research base across multiple disorders like panic, PTSD, and social anxiety.
Conclusion
As Mark, my architect patient, eventually found, the right SSRI didn’t change his personality—it cleared the scaffolding that was blocking his view. By lowering the static of his constant “what-ifs,” he was able to engage in our sessions with a clarity he hadn’t felt in years.
Anxiety is a thief of time and presence. While medication is never the entire solution, for many, it is the bridge that allows them to walk out of the “gray” and back into a life where they are in control, rather than their fear.
References
- American Psychiatric Association (APA)
- National Institute of Mental Health (NIMH)
- The Lancet
- Harvard Health
Related Posts






Subscribe to Our Newsletter
Get mental health tips, updates, and resources delivered to your inbox.
MORE from Author
Read More In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure…
In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure… We all have "up" days and "down" days. Perhaps you feel energized after a promotion or sluggish on a rainy…
We all have "up" days and "down" days. Perhaps you feel energized after a promotion or sluggish on a rainy…
 To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,…
To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,… To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…
To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…
Are you looking for a Therapist?
Connect with qualified mental health professionals who understand
bipolar disorder, mood changes, and emotional challenges.
Private • Supportive • Confidential