How Quetiapine Works: Brain Chemistry, Timeline, Sleep Effects & Safety
In my clinical practice, I often observe a specific moment of hesitation when a patient is first prescribed quetiapine (widely known by the brand name Seroquel). Because it is classified as an “atypical antipsychotic,” there is frequently a misconception that the medication is “too heavy” for their specific needs, particularly if they are struggling with bipolar depression or insomnia rather than psychosis.
However, quetiapine is one of the most versatile pharmacological tools we have in modern psychiatry. Understanding how quetiapine works is not just about memorizing a list of receptors; it is about understanding how this molecule can stabilize a dysregulated nervous system.
Whether it is used to quiet the intrusive “noise” of racing thoughts or to provide a biological floor for someone trapped in the depths of a depressive episode, its mechanism is a fascinating study in neurobiology.
What Is Quetiapine and What Is It Used For?
Before we dive into the “why,” we must establish the “what.” Quetiapine is a second-generation (atypical) antipsychotic. You will often see it labeled as quetiapine fumarate; the “fumarate” is simply the salt form that allows the medication to be stable and absorbable by the human body.
FDA-Approved Indications
The FDA has approved quetiapine for three primary conditions, each requiring a different strategy:
- Schizophrenia: To manage hallucinations and delusions.
- Bipolar Disorder: It is a first-line treatment for acute mania and bipolar depression, and as a maintenance therapy to prevent relapse.
- Major Depressive Disorder (MDD): It is used as an “adjunct” (add-on) therapy when standard antidepressants alone are insufficient.
In psychiatric practice, I often see quetiapine selected when a patient’s profile includes a “triple threat”: mood instability, high agitation, and severe insomnia. Because it addresses all three simultaneously, it can simplify a treatment plan that might otherwise require three separate medications.
You can read our full guide on What is Quetiapine
How Quetiapine Works in the Brain

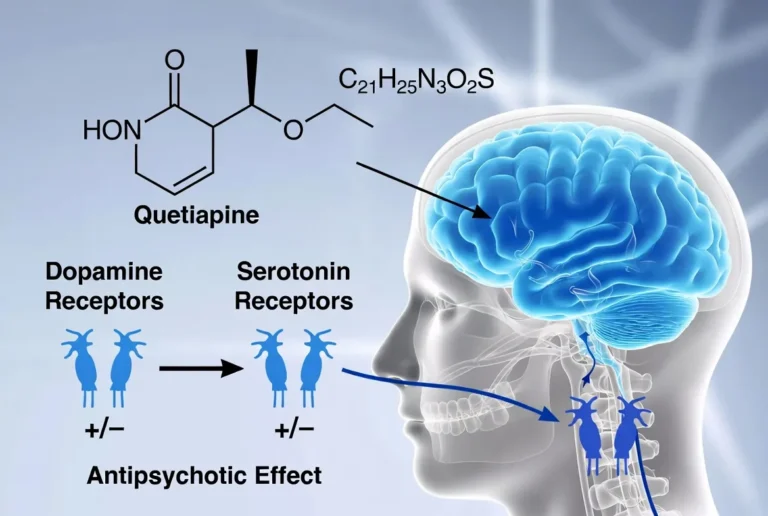
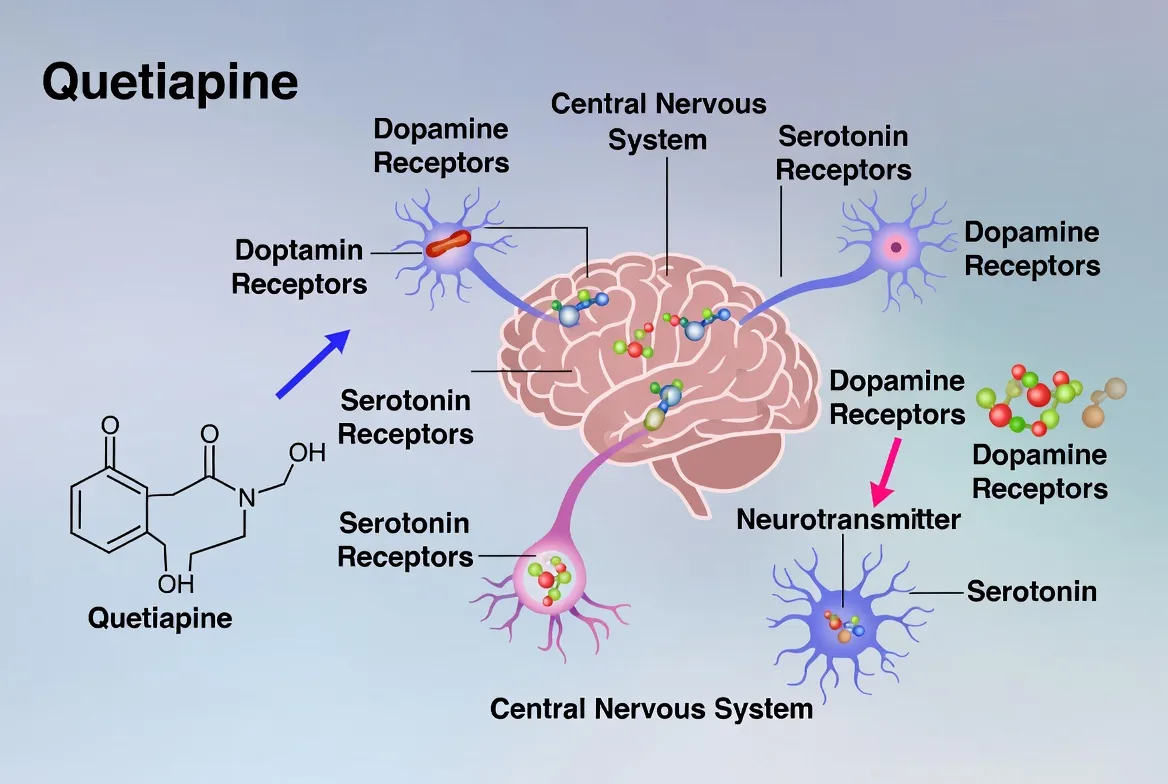
To truly understand how quetiapine works in the brain, it is helpful to view it as a pharmacological “multi-key” molecule. Most traditional medications are designed to fit seamlessly into one specific receptor “lock” to turn a neurological signal either on or off. Quetiapine, however, is a second-generation (atypical) antipsychotic that interacts with a remarkably wide array of neurotransmitter systems.
Because of this broad receptor profile, quetiapine is highly dose-dependent. At low doses, it fits comfortably into one set of locks; at medium doses, it unlocks another; and at high doses, it engages entirely different neural pathways. Here is the detailed clinical breakdown of how it alters brain chemistry.
a. Dopamine Modulation: The Anti-Manic Mechanism
In neurological states of acute mania or active psychosis, specific regions of the brain—particularly the mesolimbic pathway—are essentially flooded with excess dopamine. This overstimulation drives racing thoughts, grandiosity, and disorganized thinking.
Quetiapine acts as a D2 receptor antagonist. It wedges itself into the dopamine receptor “lock,” effectively blocking the excess dopamine from binding and overstimulating the brain. This is the primary mechanism that “calms the mind” during a manic episode.
However, unlike older typical antipsychotics (like Haloperidol) that bind to D2 receptors aggressively and permanently, quetiapine exhibits “fast-off” binding. It blocks the receptor just long enough to reduce the manic symptoms but detaches quickly enough to significantly lower the risk of severe movement disorders (extrapyramidal symptoms) and stiffness that plagued older treatments.
b. Serotonin Regulation: The Antidepressant Engine
Older antipsychotics strictly blocked dopamine, which often left patients feeling emotionally flat, lethargic, or deeply depressed. Quetiapine avoids this through its high affinity for 5-HT2A serotonin receptors.
When quetiapine blocks these specific serotonin receptors, it triggers a fascinating downstream effect: it actually increases the release of dopamine in the prefrontal cortex.
The prefrontal cortex is the brain’s command center for executive function, planning, motivation, and emotional regulation. By boosting dopamine specifically in this area, quetiapine effectively lifts the “brain fog” and profound apathy of depression.
Furthermore, as the liver breaks down quetiapine, it creates an active metabolite called norquetiapine. This metabolite acts as a potent norepinephrine reuptake inhibitor (NET inhibitor), keeping more norepinephrine available in the brain.
The combination of prefrontal dopamine release and increased norepinephrine is the biological reason quetiapine is incredibly effective for the crippling “lows” of bipolar depression.
c. Histamine Blockade: The Sedation Mechanism
Perhaps the most universally recognized aspect of quetiapine is its profound sedating effect, which is governed by the H1 histamine receptors. Histamine is an excitatory neurotransmitter that promotes wakefulness and alertness.
Quetiapine has an incredibly high affinity for H1 receptors—meaning it prefers to bind to histamine receptors before almost any other target in the brain. When you block histamine, the biological result is rapid and profound sedation.
Because the medication targets these receptors first, even a tiny “micro-dose” (like 25mg or 50mg) will saturate the H1 receptors, causing someone to feel incredibly drowsy within an hour.
This mechanism is incredibly useful for bipolar patients suffering from manic insomnia, but it is also the mechanism responsible for the notorious “Seroquel hangover” and the associated metabolic side effects, such as increased appetite and carbohydrate cravings.
d. Alpha-1 Adrenergic Blockade: The Vascular Response
Beyond its effects on mood and sleep, quetiapine interacts with the peripheral nervous system by acting as an alpha-1 adrenergic receptor antagonist.
Under normal circumstances, alpha-1 receptors help manage your vascular tone. When you stand up from a sitting or lying position, these receptors signal your blood vessels to constrict, pushing blood up to your brain to maintain your blood pressure.
Quetiapine blocks this signal. As a result, when a patient stands up quickly, the blood vessels do not constrict fast enough, leading to a temporary drop in blood pressure.
This phenomenon, known as orthostatic hypotension, is the biological reason why patients often experience sudden dizziness, lightheadedness, or an increased heart rate when standing, making careful dose titration and slow physical movements critical during the early stages of treatment.
How Quetiapine Works for Sleep
I am frequently asked, “How does quetiapine work for sleep?” or “Is quetiapine just a sleeping pill?”
While quetiapine is highly sedating, it is not FDA-approved as a primary insomnia medication. However, Seroquel for sleep is one of the most common off-label uses in psychiatry. The sedation comes primarily from the antihistamine effect mentioned above.
At a quetiapine for sleep dosage (usually 25 mg to 50 mg), the medication is essentially a very powerful antihistamine. It doesn’t yet have enough “power” at that dose to significantly alter dopamine or serotonin levels. For many patients, especially those with bipolar disorder, quetiapine improves sleep within the first few nights—long before the mood-stabilizing effects kick in.
In my practice, I once worked with a patient, “Marcus,” who was prescribed low-dose quetiapine for chronic insomnia. He was frustrated because the medication would “knock him out,” but he still felt exhausted the next day.
The Nuance: What only a practicing clinician might observe is that quetiapine can sometimes “mask” poor sleep hygiene. Marcus was taking his quetiapine and then scrolling on a high-blue-light smartphone for an hour. While the drug forced his brain into sleep, the blue light suppressed his natural melatonin and disrupted his circadian rhythm.
Once we combined the medication with a strict “digital sunset,” the quetiapine worked with his biology rather than just forcing it. His morning grogginess vanished because his brain was finally entering high-quality REM sleep.
How Quetiapine Works for Anxiety
Many patients find that quetiapine “calms the mind” in a way that traditional anti-anxiety meds (like SSRIs) do not. Is quetiapine safe for anxiety? While it is not a first-line treatment for generalized anxiety disorder, it is incredibly effective for “anxious distress” within mood disorders.
It works for anxiety by
- Reducing Hyperarousal: By blocking histamine and alpha-1 receptors, it physically slows down the “fight or flight” response.
- Slowing Intrusive Thoughts: By modulating dopamine, it can reduce the “sticky” nature of repetitive, anxious thoughts.
Unlike benzodiazepines (like Xanax), quetiapine is not considered addictive, making it a preferred choice for clinicians when treating anxiety in patients with a history of substance use or those who need 24-hour symptom coverage rather than acute, short-term relief.
How Long Before Quetiapine Works?
One of the most common frustrations in psychiatric treatment is the gap between taking the first pill and feeling “better.” How long until quetiapine works depends entirely on which symptom we are targeting.
The Quetiapine Timeline:
- Sedation (Sleep): 30 to 120 minutes. This is almost immediate.
- Acute Agitation/Anxiety: Within a few days. As the drug builds up a steady state in your blood, the “edge” begins to come off.
- Bipolar Depression: 2 to 4 weeks. It takes time for the serotonin modulation to result in neuroplasticity—the physical rewiring of the brain’s mood centers.
- Antipsychotic Effects (Schizophrenia/Mania): 4 to 6 weeks. High-dose dopamine blockade requires a consistent “soak” to fully stabilize disorganized thought patterns.
Patients often find that sleep improves in week one, but they don’t feel “happy” or “stable” until week four. Understanding this timeline is crucial for preventing patients from giving up on the medication too early.
What Happens If You Take Quetiapine?
When you begin taking quetiapine, the experience is often described as a systemic “slowing down.” Because of its high affinity for histamine receptors, the initial physical sensation is one of heavy-lidded drowsiness.
For a person in the midst of a manic episode or a “normal” person (someone without a psychiatric diagnosis), this can feel like being wrapped in a thick, pharmacological blanket.
Short-Term Physical and Cognitive Shifts
Within the first few days, you may experience:
- Reduced Mental “Static”: Many patients report that quetiapine successfully “calms the mind,” reducing the volume of intrusive or racing thoughts.
- Metabolic Shifts: You may notice a sharp increase in appetite, particularly for carbohydrates. This is a direct result of the medication’s effect on the hypothalamus and its interference with insulin sensitivity.
- Physical Relaxation: A decrease in the physical “jitteriness” often associated with anxiety or agitation.
Pros and Cons of Quetiapine
Deciding to use quetiapine involves a careful “cost-benefit” analysis between your psychiatric stability and your physical health. In my experience, for those with severe bipolar disorder, the “pro” of maintaining reality and mood stability often outweighs the “con” of side effects—but this is a deeply individual choice.
The Advantages (Pros)
- Versatility: It is a “one-stop shop” for many, treating depression, mania, and insomnia simultaneously.
- Rapid Sleep Onset: Unlike SSRIs, which can take weeks to help with sleep, quetiapine works almost immediately to restore a sleep-wake cycle.
- Non-Addictive: Unlike benzodiazepines, there is no “craving” or dopamine-driven reward loop, making it safer for long-term use in high-risk populations.
The Disadvantages (Cons)
- Weight Gain: This is the primary reason for discontinuation. It can alter lipid profiles and blood sugar levels.
- The “Seroquel Fog”: Some patients find the daytime sedation too intense, impacting their ability to operate machinery or focus at work.
- Long-Term Risks: There is a small risk of tardive dyskinesia (TD)—involuntary muscle movements—and metabolic syndrome.
| Side Effect Category | Common Symptoms | Management Strategy |
| Metabolic | Weight gain, increased blood sugar | Baseline and quarterly A1C/Lipid panels |
| Neurological | Drowsiness, or “brain fog.” | Taking the dose earlier in the evening |
| Cardiovascular | Dizziness upon standing | Hydration and slow postural changes |
| Sexual | Decreased libido | Discussion of dose adjustment or adjuncts |
Common and Low-Dose Side Effects
Even at a low dose of Seroquel (25 mg to 50 mg), the side-effect profile is not zero. It is a common misconception that low doses are “risk-free” because they aren’t being used for psychosis.
Metabolic and Sexual Nuances
Even at 25mg, quetiapine can impact your metabolism. I have had patients gain weight on low doses simply because the medication makes them “sleep-eat” or increases their appetite just before bed.
Furthermore, quetiapine side effects sexually can include a decrease in desire, though it is often less severe than the sexual dysfunction caused by standard antidepressants.
When Quetiapine Is “Not Working Anymore”
If you feel the medication has lost its efficacy, it is rarely “tolerance” in the way we see with opioids. Instead, it is often a shift in the underlying disease progression or an environmental stressor that has overwhelmed the current dosage.
In these cases, we look at neuroplasticity—has the brain adjusted its receptor density, or do we need to pivot to a different class of mood stabilizer?
Frequently Asked Questions
How long does it take for quetiapine to kick in?
For sleep, it takes 30 to 120 minutes. For mood stabilization in bipolar depression or mania, it typically takes 2 to 4 weeks for the full therapeutic effect to be felt.
Does quetiapine calm your mind?
Yes. By modulating dopamine and serotonin, quetiapine dampens the overactivity in the brain’s “salience network,” making intrusive or racing thoughts feel further away and less urgent.
Is quetiapine safe long-term?
Quetiapine is considered safe for long-term use under strict medical supervision. This includes regular monitoring of weight, blood sugar, and cholesterol to prevent metabolic syndrome.
Why is quetiapine so sedating?
It is an extremely potent H1 histamine antagonist. This means it blocks the “wakefulness” signals in the brain more effectively than many over-the-counter allergy medications.
Can quetiapine stop working?
It doesn’t “stop working” biologically, but your brain’s needs may change. If symptoms return, it usually requires a dosage adjustment or an evaluation of other lifestyle factors like stress or sleep hygiene.
Conclusion
In my years of clinical work, I have seen quetiapine act as a bridge from chaos to stability. It is a medication of profound nuance—one that requires a partnership between you and your prescriber. By understanding the “why” behind the sedation and the “how” behind the mood stabilization, you can take an active role in your recovery.
Remember, the goal of psychiatric medication is not to “numb” you, but to provide the neurochemical floor you need to engage in the work of therapy and the joy of daily life. If the side effects become a barrier to that joy, do not hesitate to discuss a new strategy with your care team.
References & Resources
- Food and Drug Administration (FDA): Seroquel Prescribing Information
- National Institute of Mental Health (NIMH): Bipolar Disorder Medications
- National Alliance on Mental Illness (NAMI): Quetiapine (Seroquel) Resource
- Mayo Clinic: Quetiapine (Oral Route) Side Effects

Related Posts




Subscribe to Our Newsletter
Get mental health tips, updates, and resources delivered to your inbox.
MORE from Author
Read More In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure…
In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure…- We all have "up" days and "down" days. Perhaps you feel energized after a promotion or sluggish on a rainy…


 To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,…
To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,… To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…
To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…


Are you looking for a Therapist?
Connect with qualified mental health professionals who understand
bipolar disorder, mood changes, and emotional challenges.
Private • Supportive • Confidential