Olanzapine (Zyprexa): A Clinical Guide to Uses, Mechanisms, and Safety
In my practice as a clinical psychologist, I often work with individuals at their most vulnerable—those navigating the disorienting “static” of schizophrenia or the exhausting oscillations of bipolar disorder.
When a psychiatrist introduces olanzapine, commonly known by the olanzapine brand name Zyprexa, the conversation usually shifts toward a delicate balance. On one hand, olanzapine is one of the most effective tools we have for quietening acute agitation and stabilizing “runaway” thoughts.
On the other hand, it is a medication that requires a high level of patient-provider collaboration due to its significant metabolic footprint.
Many patients come to me with “sticker shock,” not from the price but from the physiological changes they experience in the first few weeks.
Understanding what olanzapine is and how it interfaces with your unique biology is the first step in moving from merely “surviving” a diagnosis to actively managing your long-term wellness.
Olanzapine
Technically categorized within the olanzapine drug class of “atypical” or second-generation antipsychotics (SGAs), this medication is prized for its versatility. Unlike older “typical” antipsychotics that primarily targeted dopamine, olanzapine’s multi-receptor approach makes it a “broad-spectrum” stabilizer.
Primary FDA-Approved Uses
- Schizophrenia: It is highly effective for “positive” symptoms (hallucinations and delusions) and, to some extent, the “negative” symptoms like social withdrawal.
- Bipolar I Disorder: It is used for acute manic or mixed episodes and as a long-term maintenance therapy to prevent relapse.
- Treatment-Resistant Depression (TRD): When combined with fluoxetine (Prozac), it is used for depression that hasn’t responded to other treatments.
Off-Label and Specialized Uses
In clinical settings, we also see olanzapine use extending to the management of severe nausea in chemotherapy patients and acute agitation in emergency settings.
It is available in various strengths—olanzapine 2.5 mg, 5 mg, 10 mg, and 20 mg—allowing for precise titration. While most take it as a daily tablet, the olanzapine injection is a critical tool for rapid stabilization in acute crises.
In my experience, clinicians often start at lower doses like 2.5 mg or 5 mg to monitor how the patient’s executive function and energy levels respond before moving to higher therapeutic ranges.
Mechanism of Action: How Olanzapine Works
When patients ask, “What does olanzapine do?” they are often looking for a reason why they feel so different so quickly. To understand the “Why,” we have to look at the “receptor soup” in the brain.
Olanzapine is a “dirty drug”—not in the sense of being impure, but because it binds to a wide variety of receptors, which explains both its high efficacy and its side-effect profile.
The Dopamine-Serotonin Balance
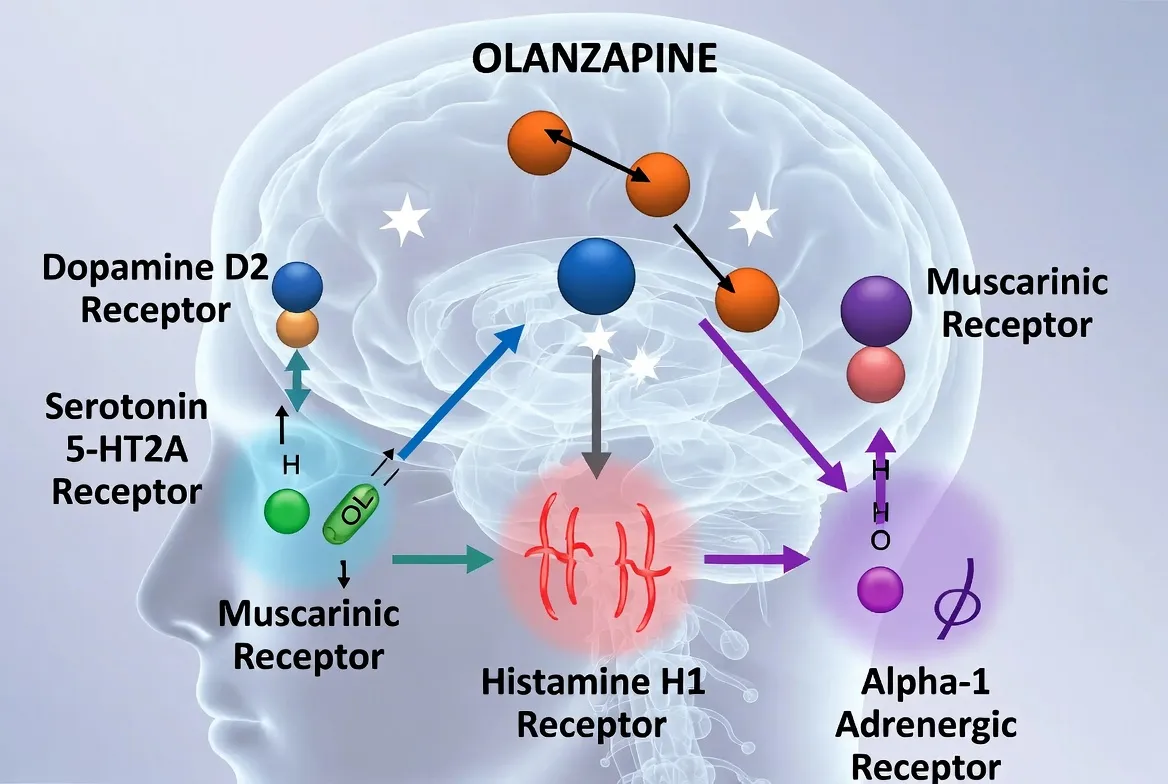
The core of how olanzapine works lies in its antagonism (blocking) of dopamine D2 and serotonin 5-HT2A receptors.
- Dopamine (D2): By blocking dopamine in the mesolimbic pathway, olanzapine quiets the “over-firing” that causes hallucinations and paranoia.
- Serotonin (5-HT2A): By blocking serotonin receptors, it actually helps release dopamine in other areas (like the prefrontal cortex), which is why it has mood-stabilizing properties and causes fewer movement disorders than first-generation drugs.
The Histamine and Muscarinic Impact (Substance over Fluff)
This is where we find the “why” behind the most common patient complaints: sedation and weight gain.
- H1 (Histamine) Receptor: Olanzapine is a potent H1 antagonist. Blocking histamine in the brain causes significant sedation and—crucially—triggers an intense craving for carbohydrates. This is the biological “hunger switch” that explains why olanzapine causes weight gain. It isn’t just about “willpower”; the drug is telling the brain it is starving.
- M3 (Muscarinic) Receptor: Its action here interferes with insulin signaling. Even before a patient eats more, the drug can begin to alter how the body processes glucose, leading to metabolic shifts.
- Alpha-1 Adrenergic: Blocking these receptors can cause “orthostatic hypotension”—that dizzy feeling you get when standing up too fast.
Understanding this receptor profile helps patients realize that their side effects aren’t “in their head”—they are a direct result of the medication’s powerful binding profile. As a psychologist, I use this information to help patients foster neuroplasticity through behavioral changes.
If we know the drug is artificially stimulating appetite, we can implement “pre-emptive” dietary structures to protect the patient’s metabolic health.
In my practice, I’ve observed a specific nuance regarding sleep hygiene. Because olanzapine is such a strong sedative, patients often rely on it to “knock them out.”
The Nuance: I once worked with a patient who took her dose at midnight but needed to be at work by 8:00 AM. She was gaining weight rapidly. We discovered that her “morning grogginess” led her to skip breakfast and binge on high-sugar snacks by noon to “wake up” her brain.
By moving her dose to 8:00 PM, she cleared the peak sedation by morning, allowing her to start the day with a protein-heavy meal. This one shift in timing stabilized her blood sugar and halted her weight gain. Sleep timing isn’t just about rest; it’s about metabolic control.
Dosing and Administration
The olanzapine dosage is never “one size fits all.” It is a delicate titration based on the severity of symptoms and the patient’s body chemistry.
- Schizophrenia & Bipolar Mania: Typically starts at 5 mg to 10 mg, with a target range of 10 mg to 20 mg per day.
- Depression (Combined with Prozac): Often starts much lower, around 2.5 mg or 5 mg.
- Special Populations: The elderly or those with hepatic (liver) impairment often stay on the lower end (olanzapine 2.5 mg) because their bodies clear the drug more slowly.
Administration Tips
I always advise taking olanzapine at bedtime. Because the peak plasma concentration occurs about 6 hours after taking it, a 9:00 PM dose ensures you are in your deepest sleep when the drug is most potent, potentially reducing daytime “brain fog.”
Regarding safety, patients with porphyria often worry about medication triggers. Fortunately, the safe status of olanzapine-induced porphyria is generally accepted in medical literature, though liver enzymes should still be monitored.
Side Effects and Safety
The conversation about olanzapine side effects must be handled with candor. While it is a life-saving medication, ignoring its physical impact can lead to treatment non-adherence.
The Metabolic Challenge
The “major side effect of olanzapine” for most is weight gain and the risk of metabolic syndrome. It is not uncommon for a patient to gain 10-15 pounds in the first month.
- Monitoring: Clinicians must track waist circumference, fasting glucose, and lipid panels.
- Management: I often work with patients on “mindful eating” techniques to counteract the drug-induced “munchies.”
Side Effect Comparison Table
| Side Effect | Frequency | Clinical Context |
| Sedation | Very High | Most intense in the first 2 weeks. |
| Weight Gain | High | Direct result of H1 and M3 receptor binding. |
| Dry Mouth | Common | Anticholinergic effect; hydration is key. |
| Orthostatic Hypotension | Moderate | Risk of dizziness upon standing. |
| EPS (Tremors) | Low | Much lower risk than older antipsychotics. |
Mark (anonymized) was a 30-year-old with bipolar I who was terrified of olanzapine because of the weight gain he saw in online forums. However, his mania was becoming dangerous. We used a “collaborative monitoring” approach. Instead of just “taking the pill,” Mark tracked his steps and his “hunger levels” daily.
When he noticed the carb cravings hitting around 10:00 PM (two hours after his dose), we implemented a therapeutic intervention: a “pre-planned evening meal” high in fiber and healthy fats taken with the medication.
This satiety-first approach helped him bypass the midnight snack raids. Mark successfully stabilized his mood on 10 mg of olanzapine without the feared weight gain, proving that with the right psychological tools, we can manage even the most “metabolic” medications.
Pharmacokinetics: How Long Does It Take to Work?
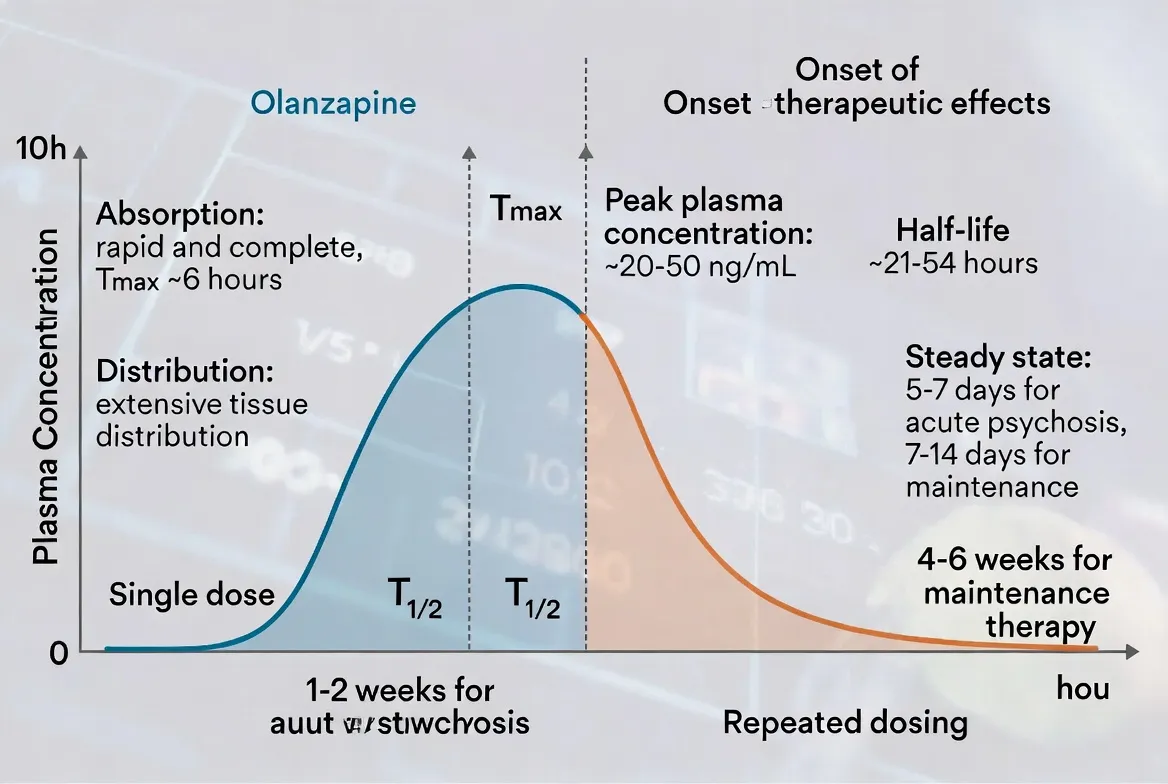
One of the most common points of frustration in my practice is the “waiting game.” Patients starting olanzapine 5 mg or 10 mg often want to know exactly how long it takes for olanzapine to work for their specific symptoms. The answer depends entirely on what we are trying to treat.
The Timeline of Relief
- Sedation and Anxiety (Hours to Days): Because of its potent antihistamine and alpha-adrenergic blocking effects, patients often feel “calmer” or sleep better within the first 24 to 48 hours.
- Acute Mania (1–2 Weeks): For bipolar episodes, significant mood stabilization usually begins within the first week of consistent dosing.
- Psychotic Symptoms (2–6 Weeks): For schizophrenia, the “heavy lifting” of clearing hallucinations and delusions takes longer. It requires reaching a “steady state” in the blood—which takes about 5 to 7 days—and then allowing the brain’s receptors to adapt over several weeks.
Half-Life and Metabolism
The olanzapine half-life is approximately 30 hours. This is relatively long, meaning the drug stays in your system for a significant amount of time.
- The Benefit: If you accidentally miss a dose by a few hours, the levels in your blood won’t drop off a cliff.
- The Factor of Smoking: A nuance many patients find surprising is that smoking cigarettes can actually speed up the metabolism of olanzapine (via the CYP1A2 enzyme). If a patient suddenly stops smoking while on olanzapine, their blood levels of the medication can rise significantly, leading to increased side effects.
Withdrawal and Drug Interactions
Stopping olanzapine is not as simple as putting the bottle away. While it is not a “controlled substance” like a benzodiazepine, it creates a significant chemical shift in the brain that requires a graceful exit.
Olanzapine Withdrawal
If you stop taking olanzapine suddenly, you may experience “rebound” symptoms. These aren’t just a return of your original illness; they are a physiological reaction to the sudden absence of the drug.
- Symptoms: Intense insomnia, nausea, sweating, and extreme irritability.
- The Rebound Effect: Because your dopamine receptors have been “blocked,” they may become hypersensitive. A sudden stop can lead to a “rebound psychosis” that is sometimes more intense than the original symptoms.
- Tapering: In my clinical experience, I recommend a slow taper over several weeks, reducing the dose in small increments (e.g., from olanzapine 10 mg to 7.5 mg, then 5 mg) to allow the brain to recalibrate.
Key Drug Interactions
- CNS Depressants: Combining olanzapine with alcohol or opioids significantly increases the risk of severe respiratory depression and extreme sedation.
- Blood Pressure Meds: Because olanzapine can lower blood pressure (orthostatic hypotension), combining it with antihypertensives requires careful monitoring to prevent fainting.
Frequently Asked Questions
Is 20 mg olanzapine a high dose?
Yes, olanzapine 20 mg is generally considered the upper limit of the standard therapeutic range. Doses higher than this are rarely used and require specialized clinical justification due to increased metabolic risks.
Does olanzapine make you sleepy?
Yes, sedation is one of the most common early side effects. Most patients take their dose at night to turn this side effect into a benefit for sleep.
Is olanzapine a mood stabilizer?
While technically an antipsychotic, it is very effective as a mood stabilizer, particularly for treating and preventing manic episodes in bipolar I disorder.
Is olanzapine the same as Xanax?
No. Xanax (alprazolam) is a benzodiazepine used for short-term anxiety. Olanzapine is an antipsychotic used for long-term stabilization of thought and mood disorders.
How long before olanzapine works for sleep?
For sleep and acute agitation, you may feel the effects within 1 to 2 hours of the first dose. However, it is not recommended as a first-line treatment for simple insomnia.
Conclusion
Olanzapine is a powerful ally in the treatment of complex mental health conditions, but it is an ally that demands respect. Its ability to “quiet the storm” of mania and psychosis is nearly unparalleled, but it requires a proactive approach to physical health and a patient-centered titration strategy.
In my work, I’ve seen that the most successful outcomes occur when the patient is not just a passive recipient of the medication but an active manager of their lifestyle.
By understanding the olanzapine side effects, monitoring metabolic markers, and ensuring a slow, guided taper when necessary, you can harness the benefits of this medication while protecting your long-term health. You deserve a life that is both stable and vibrant.
References & Resources
- National Institute of Mental Health (NIMH): Bipolar Disorder Medications
- National Alliance on Mental Illness (NAMI): Olanzapine (Zyprexa) Profile
- FDA.gov: Zyprexa (olanzapine) Prescribing Information
- Bipolar Lives: Olanzapine (Zyprexa) Side Effects and Management

Related Posts




Subscribe to Our Newsletter
Get mental health tips, updates, and resources delivered to your inbox.
MORE from Author
Read More In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure…
In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure…- We all have "up" days and "down" days. Perhaps you feel energized after a promotion or sluggish on a rainy…


 To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,…
To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,… To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…
To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…


Are you looking for a Therapist?
Connect with qualified mental health professionals who understand
bipolar disorder, mood changes, and emotional challenges.
Private • Supportive • Confidential