Is Borderline Personality Disorder the Same as Bipolar? Differences, Symptoms & How to Tell

When experiencing rapid shifts in mood, intense emotions, or turbulent relationships, many people find themselves searching for answers online. Two of the most common diagnoses that appear in these searches are Bipolar Disorder and Borderline Personality Disorder (BPD). Because both conditions involve emotional instability, many patients and even some general practitioners ask: Is borderline personality disorder the same as bipolar?
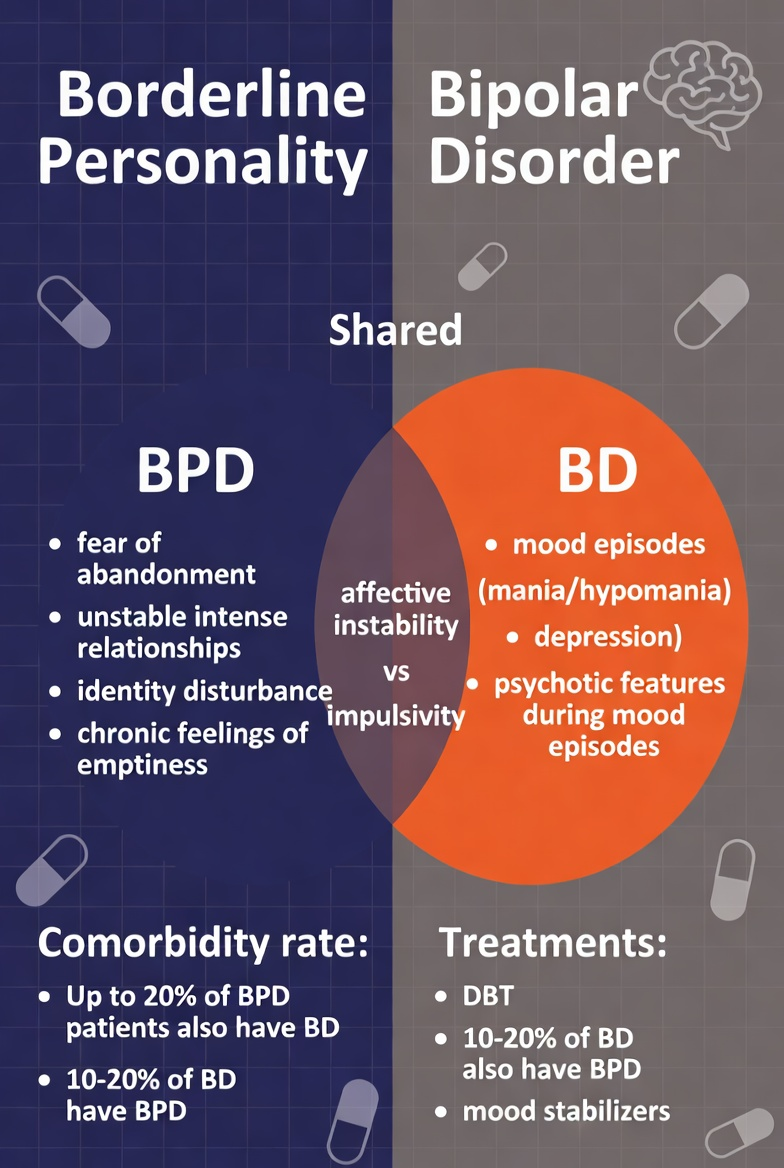
The short answer is no. While they share overlapping symptoms—such as impulsivity and intense emotional states—they are fundamentally different categories of mental illness. Bipolar disorder is classified as a mood disorder, primarily driven by biological and chemical shifts in the brain. Borderline Personality Disorder is classified as a personality disorder, characterized by long-standing patterns of how a person relates to themselves and others, often rooted in early developmental trauma or emotional dysregulation.
Confusing the two is not just a matter of semantics; it has significant clinical implications. The treatment for bipolar disorder often relies heavily on medication to stabilize brain chemistry, whereas the “gold standard” for BPD is intensive psychotherapy. Understanding the nuances of whether bipolar disorder is the same as borderline personality disorder is the first step toward receiving the correct diagnosis and, ultimately, the right treatment.
Bipolar vs BPD at a Glance
For those looking for a rapid comparison, the difference between bipolar and borderline comes down to the “nature” and “duration” of mood shifts.
- Bipolar Disorder: Mood shifts occur in “episodes” that usually last for days, weeks, or even months. These shifts are often independent of external events.
- Borderline Personality Disorder: Mood shifts are “reactive,” occurring in response to external triggers (like a perceived rejection). These “emotional storms” may last only a few hours.
Core Differences Table
| Feature | Bipolar Disorder | Borderline Personality Disorder |
| Category | Mood Disorder | Personality Disorder |
| Mood Triggers | Often spontaneous/biological | Almost always external/interpersonal |
| Mood Duration | Days to weeks (Episodes) | Minutes to hours (Reactivity) |
| Core Issue | Energy and activity levels | Relationships and self-image |
Bipolar Disorder Explained
To understand the differences between bipolar and BPD, we must first define what bipolar disorder actually looks like. It is characterized by extreme fluctuations in mood, energy, and the ability to function. These fluctuations are divided into two main poles: mania (or hypomania) and depression.
Bipolar I vs. Bipolar II
In Bipolar I, individuals experience “full mania,” which can include grandiosity, a total lack of sleep for days, and sometimes psychosis. In Bipolar II, the high is less extreme—called hypomania—but the depressive episodes are often more frequent and debilitating. Bipolar type 2 vs BPD is the most common area of confusion because hypomania can sometimes look like the high energy of a BPD emotional surge.
Episode Duration and Cycling
A hallmark of bipolar disorder is the “episode.” Unlike the momentary anger of BPD, a bipolar manic or depressive episode represents a sustained change from an individual’s baseline. Even in “rapid cycling” bipolar, these shifts typically take days to manifest and resolve, rather than shifting multiple times within a single afternoon.
Borderline Personality Disorder Explained
Borderline Personality Disorder (BPD) is centered on a pervasive pattern of instability in interpersonal relationships, self-image, and affect. While borderline personality disorder symptoms involve mood changes, they are distinct from the biological “cycles” of bipolar.
Emotional Dysregulation
The primary struggle in BPD is the inability to regulate emotions. If a person with BPD perceives a threat—such as a friend not texting back—they may experience an immediate, “10-out-of-10” emotional reaction. This is often followed by a “shame spiral” once the emotion subsides.
Fear of Abandonment and Identity
Unlike bipolar disorder, BPD is heavily tied to the presence of others. The hypomania, borderline personality disorder, andconfusion usually stem from the “euphoria” a person with BPD feels when a relationship is going well. However, BPD also involves a fragmented sense of self; the person may change their goals, values, and even personality traits depending on who they are with to avoid being alone.
Borderline Personality Disorder vs Bipolar Disorder: Core Differences
When comparing borderline personality disorder vs bipolar disorder, clinicians look at several “differentiators” to ensure the patient isn’t misdiagnosed.
1. Mood Triggers vs. Spontaneous Episodes
In BPD, moods are highly reactive. If you win an award, you are ecstatic; if you receive a critique, you are suicidal. In bipolar disorder, a person might wake up in a deep depression despite having a “perfect” life, or enter a manic phase despite facing a tragedy. The trigger is internal and chemical rather than external and social.
2. Duration of Mood Changes
The “speed” of the shift is the biggest clue. A person with BPD can go from despair to joy three times in a single lunch date. A person with bipolar disorder stays in one “state” for a significant period. Even the fastest-shifting bipolar patients rarely cycle as quickly as a person with BPD.
3. Relationship Patterns
In BPD, relationships are often characterized by “splitting”—viewing someone as either all good or all bad. This is driven by a deep fear of abandonment. While bipolar symptoms can strain relationships (due to manic overspending or depressive withdrawal), the core of the disorder is not an obsession with the relationship itself.
4. Response to Treatment
This is perhaps the most practical difference between bipolar and borderline. Bipolar disorder usually responds well to mood stabilizers like Lithium or anticonvulsants. BPD, however, rarely responds to medication alone. Instead, Dialectical Behavior Therapy (DBT) is the primary treatment, focusing on teaching the patient how to manage their emotions through skill-building.
Bipolar 2 vs BPD: Why These Two Are Most Often Confused
The comparison between bipolar 2 vs bpd is the “frontier” of diagnostic difficulty. Because Bipolar II involves hypomania—which is less disruptive than full mania—it can look remarkably like the “high-functioning” emotional reactivity of BPD.
Hypomania vs. Emotional Reactivity
Hypomania involves a sustained period (at least four days) of elevated mood, decreased need for sleep, and increased productivity. In BPD, an “up” mood is usually a reaction to a positive interpersonal event and rarely lasts four days straight without interruption.
Misdiagnosis Risks
Women are statistically more likely to be diagnosed with BPD, while men are often diagnosed with bipolar disorder. This gender bias in the medical community can lead to bipolar type 2 vs. BPD misidentification, leaving patients with the wrong treatment plan. If a person with BPD is treated only with Lithium, their relationship struggles and fear of abandonment remain unaddressed.
Borderline Personality Disorder vs Bipolar 1
When looking at borderline personality disorder vs bipolar 1, the distinction is usually clearer. The “Full Mania” of Bipolar I is a dramatic clinical event.
- Hospitalization: Bipolar I mania often leads to hospitalization because the person loses touch with reality or becomes a danger to themselves through reckless behavior (spending thousands of dollars, starting a business overnight, or not sleeping for a week).
- Psychosis: Psychosis (hallucinations or delusions) can occur in Bipolar I mania. While BPD can involve “stress-related paranoia,” it rarely reaches the level of sustained delusional thinking found in Bipolar I.
- The “Crash”: The depressive crash following a Bipolar I manic episode is often vegetative—the person may not be able to get out of bed for weeks. BPD depression is usually “active,” involving high levels of emotional pain and self-harm urges.
Bipolar vs Borderline Chart
To help visualize these differences for diagnostic clarity, use the following chart as a reference point.
Comparison of Clinical Indicators
| Clinical Indicator | Bipolar Disorder | Borderline Personality Disorder (BPD) |
| Typical Onset | Late teens to early 20s | Mid-to-late teens |
| Mood Duration | Weeks or Months | Hours or Days |
| Sleep Patterns | Significantly decreased need for sleep during mania | Normal sleep, or sleep disrupted by anxiety/nightmares |
| Self-Image | Usually stable, but grandiose during mania | Chronically unstable; “Who am I?” |
| Stability | Often “baseline” and stable between episodes | Persistent emotional vulnerability |
| Primary Treatment | Pharmacotherapy (Mood Stabilizers) | Psychotherapy (DBT / MBT) |
Which Is Worse: Bipolar or BPD?
When patients or family members ask if bipolar or bpd worse, they are usually searching for a way to quantify the immense suffering both conditions cause. From a clinical perspective, “worse” is not a useful term, as both can be life-threatening and deeply disruptive to one’s quality of life. However, they present different types of challenges.
The Struggle of BPD vs. Bipolar
In which is worse, bipolar or BPD Reddit threads, many users point out that BPD is often characterized by “chronic” suffering. Because BPD is a personality disorder, emotional vulnerability is present almost every day. In contrast, Bipolar disorder is “episodic.” A person with bipolar disorder may have months or years of high-functioning stability between episodes, whereas someone with BPD often feels they are constantly “on fire” emotionally.
Stigma and Mortality
Historically, BPD has carried a heavier social stigma, even among mental health professionals, leading to it being called one of the hardest mental illnesses to live with. However, both conditions carry a high risk of suicide. Approximately 70% of people with BPD will attempt suicide at least once, and the suicide completion rate for Bipolar disorder is roughly 15 to 20 times higher than that of the general population. Ultimately, the “worst” condition is whichever one is currently untreated.
Can Someone Have BPD and Bipolar at the Same Time?
It is entirely possible to have a “dual diagnosis.” In fact, research suggests that roughly 20% of people with Bipolar II also meet the criteria for BPD. When this occurs, it is referred to as comorbidity.
How Symptoms Interact
When you have BPD and bipolar disorder, the symptoms can mask one another. For example, a manic episode might be triggered by a BPD interpersonal conflict, or a BPD “fear of abandonment” might be significantly amplified during a bipolar depressive slump.
This makes the diagnostic process much more complex, as the clinician must determine what part of the mood shift is chemical (Bipolar) and what part is reactive (BPD).
Treatment Implications
Treatment for comorbid cases must be integrated. Stabilizing the mood with medication (for Bipolar) is often necessary before the patient can gain enough emotional regulation to participate effectively in DBT (for BPD).
Triggers, Stability & “Seeming Normal.”
A common point of confusion for loved ones is why a person can seem perfectly fine one moment and be in a total crisis the next.
What Triggers BPD?
Unlike the biological shifts of Bipolar, what triggers BPD is almost always “relational.” This can include a perceived slight, a delayed text, a disagreement, or a significant life change like a breakup. Because these triggers are often subtle to an outsider, the reaction can seem disproportionate or “out of nowhere.”
Masking and High-Functioning BPD
Can someone with BPD seem normal? Yes. Many individuals practice “quiet BPD” or “masking,” where they turn their intense emotions inward rather than lashing out. In these cases, the person may be highly successful at work or school, while experiencing a private hell of self-loathing and emotional turbulence once they are behind closed doors.
Is BPD a Disability? Is Bipolar a Disability?
From a legal and functional standpoint, both conditions can qualify as disabilities if they significantly impair your ability to perform “Substantial Gainful Activity.”
- Bipolar Disorder: Often qualifies for Social Security Disability (SSDI) because the length of the episodes (weeks/months) makes it impossible to maintain a standard work schedule.
- BPD: Is having BPD a disability? Yes, it is recognized under the Americans with Disabilities Act (ADA). However, it is often harder to win a disability claim for BPD alone because the symptoms are considered “reactive” rather than “persistent” in the way a 6-month depressive episode is.
Workplace accommodations for both might include flexible scheduling, a quiet workspace, or the ability to take “mental health days” during acute symptomatic periods.
BPD vs. Bipolar vs. Schizophrenia
Sometimes, the intensity of these conditions leads to a comparison with Schizophrenia. It is important to define the boundaries between these three.
- Bipolar: A mood disorder. Psychosis (hallucinations/delusions) only happens during extreme mood peaks or troughs.
- BPD: A personality disorder. “Paranoia” or “dissociation” can happen under extreme stress, but it is usually fleeting.
- Schizophrenia: A “thought disorder.” Psychosis is a primary feature and can occur regardless of whether the person is happy or sad.
Psychology Today, Media & Public Confusion
If you read Psychology Today borderline vs bipolar articles, you will see a recurring theme: the media often uses “Bipolar” as a catch-all term for anyone with a temper, and “Borderline” as a slur for anyone who is “difficult” in a relationship.
This oversimplification causes real harm by discouraging people from seeking the specific help they need. Bipolar is not “moodiness,” and BPD is not “being toxic.” They are serious medical and psychological conditions that require scientific intervention.
Do I Have BPD or Bipolar? (Self-Refection)
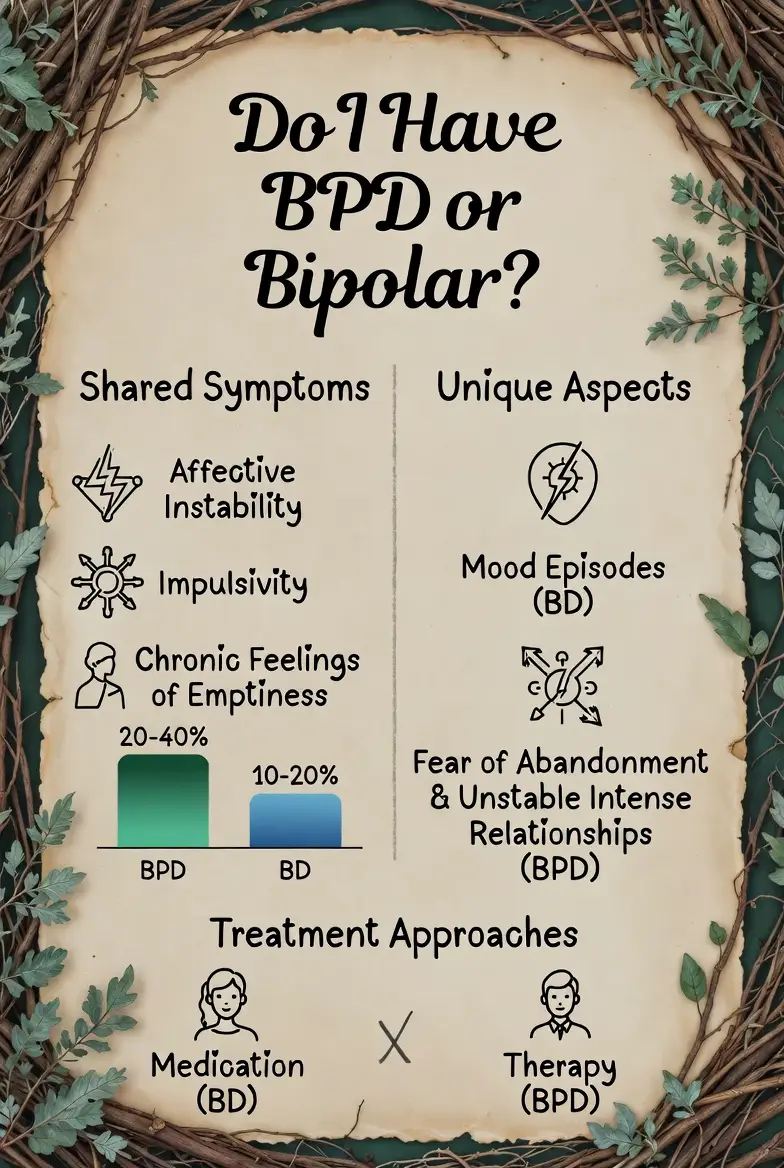
While only a psychiatrist or psychologist can provide a diagnosis, you can use these self-reflection questions to prepare for a professional consultation. This is not a do I have BPD or bipolar quiz, but a guide for self-observation.
- Do my moods change based on what people say to me, or do they seem to have a life of their own? (Reactive = BPD; Spontaneous = Bipolar)
- How long do my “highs” last? (Hours = BPD; Days/Weeks = Bipolar)
- When I am upset, it’s usually because I’m afraid someone is leaving me. (Yes = BPD)
- Do I experience periods where I don’t need to sleep for several days but still feel energetic? (Yes = Bipolar)
- Does my sense of “who I am” change depending on who I am dating or hanging out with? (Yes = BPD)
Detailed Breakdown of Emotional Regulation vs. Biological Rhythms
To deepen our understanding of whether borderline personality disorder is the same as bipolar disorder, we must look at the underlying mechanisms of how the brain processes “stability.” In a neurotypical brain, there is a certain “emotional baseline.”
When something good happens, the mood rises; when something bad happens, it falls. However, the brain eventually pulls the mood back to the center.
The “Broken Thermostat” of BPD
In Borderline Personality Disorder, the brain’s “emotional thermostat” is effectively broken. When a person with BPD experiences a trigger, their emotion doesn’t just rise; it spikes to a point of agony. Because they lack the internal “cooling system” to bring that emotion back down, they often resort to impulsive behaviors (self-harm, substance use, or lashing out) to try to stop the pain. This is why BPD is often described as “emotional third-degree burns.”
The “Shifting Tides” of Bipolar
In Bipolar Disorder, the issue isn’t necessarily a reaction to a single event, but a shift in the “sea level” of the brain’s energy. During a manic episode, the baseline itself is elevated. Even if something sad happens, the manic energy may simply override it.
During a depressive episode, the baseline is so low that even a winning lottery ticket might not spark a smile. It is a state of being that colors every experience, rather than a reaction to a specific experience.
Misdiagnosis in Women: The Intersection of Gender and Clinical Bias
A significant factor in the bipolar 2 vs. BPD confusion is clinical bias. Historically, women have been disproportionately diagnosed with Borderline Personality Disorder, while men with similar symptoms are often diagnosed with Bipolar or Intermittent Explosive Disorder.
- The “Hysteria” Legacy: There is a long-standing (and harmful) medical legacy of labeling women’s emotional distress as “personality-based” or “manipulative,” which are stigmas often attached to BPD.
- Hormonal Overlap: For women, Premenstrual Dysphoric Disorder (PMDD) can cause rapid mood shifts that mimic BPD or ultra-rapid cycling Bipolar.
- The Danger of Mislabeling: If a woman with Bipolar II is misdiagnosed as BPD, she may be put through years of therapy without the mood stabilizers she needs to stop her biological cycles. Conversely, if a woman with BPD is labeled Bipolar, she may be over-medicated while her underlying trauma remains unaddressed.
Navigating Treatment: DBT vs. Medication
Understanding the difference between bipolar and borderline becomes a matter of life and death when choosing a treatment path.
Dialectical Behavior Therapy (DBT) for BPD
DBT was specifically created by Dr. Marsha Linehan to treat BPD. It focuses on four key pillars:
- Mindfulness: Learning to be present in the moment without judgment.
- Distress Tolerance: Learning how to survive an “emotional storm” without making things worse.
- Emotion Regulation: Learning how to change the emotions that you want to change.
- Interpersonal Effectiveness: Learning how to ask for what you need and say “no” while maintaining self-respect and relationships.
Medication Protocols for Bipolar
For Bipolar, the goal is “prophylaxis”—preventing the next episode.
- Lithium: The classic mood stabilizer.
- Anticonvulsants: Like Lamictal or Depakote, which help “level out” the brain’s electrical activity.
- Antipsychotics: Used to manage mania or “mixed features.”
Frequently Asked Questions
Is borderline personality disorder the same as bipolar?
No. Bipolar is a mood disorder (biological cycles); BPD is a personality disorder (interpersonal/emotional patterns).
Can you have BPD and bipolar?
Yes. Comorbidity is common, affecting about 20% of Bipolar II patients.
What is the hardest mental illness to live with?
Both are ranked among the highest for emotional distress, but BPD is often cited due to the chronic nature of the pain and the stigma attached to it.
Can someone with BPD seem normal?
Yes, many individuals “mask” their symptoms, appearing high-functioning while struggling intensely in private.
Conclusion
Whether you are navigating the highs of Bipolar I or the emotional storms of BPD, the most important thing to remember is that neither diagnosis is a life sentence. The confusion between these two conditions is real, but once you peel back the layers of “mood swings,” the distinct patterns of each begin to emerge.
If you are struggling, don’t settle for a “vague” diagnosis. Seek a specialist who understands the nuances of personality vs. mood. With the right combination of medication for Bipolar and specialized therapy like DBT for BPD, you can move from a life of “managing symptoms” to a life of genuine stability and joy.
Authoritative References
- National Institute of Mental Health (NIMH) – Bipolar Disorder
- National Education Alliance for Borderline Personality Disorder (NEA.BPD)
- Mayo Clinic – Personality Disorders vs. Mood Disorders
- The Stability Network – Living with Bipolar
- Psychology Today – Misdiagnosis of BPD and Bipolar

Related Posts



Subscribe to Our Newsletter
Get mental health tips, updates, and resources delivered to your inbox.
MORE from Author
Read More In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure…
In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure…- We all have "up" days and "down" days. Perhaps you feel energized after a promotion or sluggish on a rainy…


 To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,…
To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,… To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…
To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…


Are you looking for a Therapist?
Connect with qualified mental health professionals who understand
bipolar disorder, mood changes, and emotional challenges.
Private • Supportive • Confidential