Lithium – How Much Do You Really Know

Lithium medication is still the most researched and proven treatment for bipolar disorder. So, why does it seem as though lithium is prescribed less and less?
My message is simple – I know lithium is not for everyone, but all my experience and research has convinced me that everyone should try it first to see. It has the most research, best track record and experts like Kay Redfield Jamison, psychiatric professor at Johns Hopkins and world renowned bipolar author and scholar (and who uses lithium herself), continues to explain lithium is still the gold standard in bipolar care.
However, bipolar treatment regimens should be tailored for the individual by a specialized physician.
My only side effect issue was with weight gain, which can be overcome by eating in a way which minimizes mood swings and avoids physical symptoms of bipolar such as metabolic syndrome, high blood pressure, diabetes, and so forth: The Bipolar Diet
What Is Lithium and Why Is It Prescribed?
Lithium is not a complex, lab-synthesized molecule; it is an element found on the periodic table (Li). In medicine, it is typically prescribed as lithium carbonate (capsules/tablets) or lithium citrate (liquid).
FDA-Approved Uses
The FDA has approved lithium for the treatment of acute manic episodes and as a maintenance therapy to prevent future episodes in Bipolar Disorder. It is uniquely effective because it addresses both “poles” of the illness, though its strength lies in curbing mania and preventing the “switch” into depression.
Off-Label Contexts
Beyond bipolar disorder, clinicians often prescribe lithium “off-label” to augment antidepressants in patients with Major Depressive Disorder (MDD) who haven’t responded to traditional SSRIs. It is also used in rare cases for cluster headaches or to manage aggressive behavior in specific neurological conditions.
The “Gold Standard” Status
Why is a drug discovered for psychiatry in 1949 still the preferred first-line treatment in 2026? The answer is simple: efficiency. Research consistently shows that lithium is more effective at preventing relapse and reducing suicidal ideation than modern alternatives like Depakote or Zyprexa. It is the only psychiatric medication proven to have a direct anti-suicidal effect, independent of its mood-stabilizing properties [1].
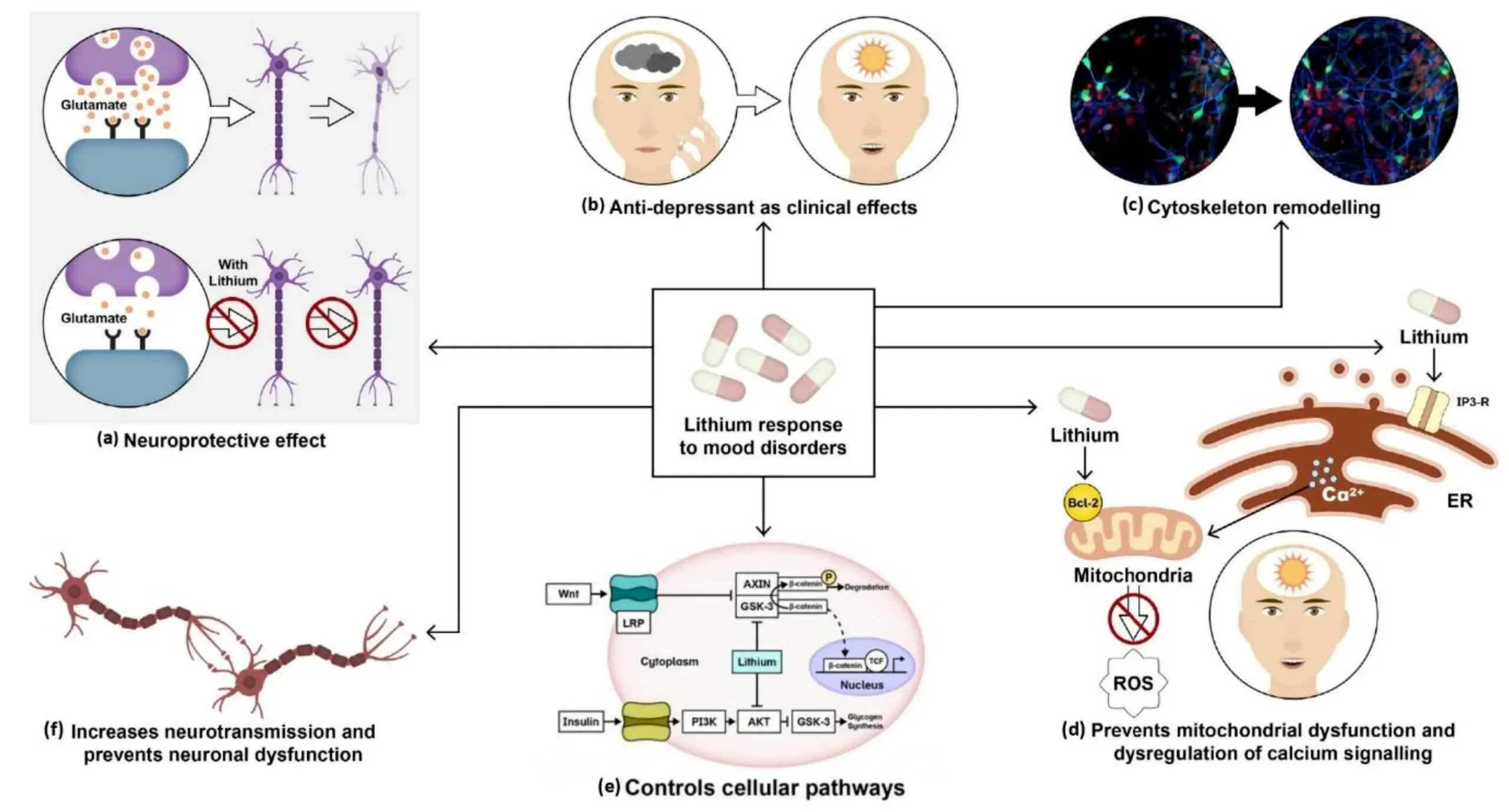
How Does Lithium Work?

In 1998, University of Wisconsin researchers found that lithium keeps the quantity of the neurotransmitter glutamate stable and at optimal levels. Dr. Lowell Hokin, a University of Wisconsin professor of pharmacology, theorized that lithium works to control bipolar because of this stabilizing effect on glutamate receptors.
This does not seem to be the whole story of why lithium is effective and it does not explain why other mood stabilizers, that do not target glutamate, can also help.
All we can say for sure is that lithium decreases abnormal activity in the brain by correcting what are probably biochemical imbalances caused by genetics.
How Does Lithium Make You Feel When You First Start?
The “induction phase” (the first 1 to 3 weeks) is the most challenging part of the journey. If you are wondering how does lithium make you feel when you first start, you should prepare for a period of physical adjustment.
Common sensations during the first two weeks include:
- Mild Nausea: Your stomach needs time to adjust to the mineral salt.
- Increased Thirst: Lithium affects how your kidneys process water, leading to a “dry mouth” feeling.
- The “LITHIUM Tremor”: A fine shakiness in the hands is very common early on.
- Drowsiness: You may feel a bit “heavy” or sleepy as your brain chemistry recalibrates.
This is why blood levels matter immensely during the start. We check your blood frequently to ensure your dose is high enough to work but low enough to avoid toxicity. Most of these early side effects dissipate once your body reaches a “steady state.”
What Happens If a Non-Bipolar Person Takes Lithium?
There is a common misconception that lithium is a general “calming drug” or a sedative. This leads people to ask, “what does lithium do to a normal person?” or “what happens if a non-bipolar person takes lithium?“
The Absence of a “High”
In a “normal” brain (one without the biochemical imbalances of bipolar disorder), lithium usually does very little to affect mood. It does not provide a “high,” it is not addictive, and it won’t make a healthy person feel “better.”
The Physical Toll
However, a non-bipolar person would still experience all the physical side effects. They would experience the thirst, the potential for kidney strain, and the thyroid interference without any of the psychiatric benefits. Therefore, taking lithium without a diagnosis is clinically useless and physically risky. It is not a “supplement”; it is a precision tool for a specific neurological “brokenness.”
My Own Lithium Experience
1. Insufficient usage of lithium
Despite all the misinformation, stigma and stereotypes, it is still the first line treatment for several types of bipolar disorder / manic depression.
2. Lithium use in acute mania and maintenance therapy
The truth is that lithium is cheap, effective, proven, and safe.
There is a lot of mystique around lithium, but in reality it is a natural salt – a simple mineral. It is ironic that so many folks resist taking lithium, insisting they want a “natural” approach. Lithium is actually as natural as it gets – it just happens to be one of the most effective bipolar medications.
Sadly, many people who could benefit from the oldest, best researched, most natural and most proven bipolar treatment are discouraged by a lot of negative half-truths and myths – many propagated online by people who are out to profit from their own products.
Everyone has different treatment needs. Many people do better on other leading bipolar medications such as Depakote or Lamictal.
However despite Depakote, the number one prescribed bipolar drug in the US, a number of studies have shown that lithium is THREE TIMES more effective in preventing suicides. Lithium use has been shown to be associated with an 87% less likelihood of suicide when compared to placebo.
3. Lignificantly less suicides with lithium vs. placebo, odds ratio (OR) 0.13
Major clinical reviews, including a seminal Cochrane-style meta-analysis in The BMJ, found that Lithium is profoundly effective at preventing the unthinkable.
In these studies, patients on Lithium had an Odds Ratio (OR) of 0.13 for suicide compared to those on a placebo. To translate that into human terms: it represents an 87% reduction in risk.
Think of it like this: If you were standing in a storm where 100 people were being swept away, Lithium acts like a reinforced anchor that keeps all but 13 of them grounded. It doesn’t just “stabilize” your mood; it specifically targets the biological “impulse-aggression” circuitry in the brain, providing a safety net that other medications simply don’t offer. It is the only psychiatric drug with this level of proven, direct anti-suicidal property.
4. Lithium medication saved my life.
Many people whose lives could easily be transformed from bipolar hell resist this cheap and effective treatment, often due to nothing but myths and half-truths. I know because I was one of them!
I should have done my homework. You see, modern lithium treatment involves lower doses and therefore fewer side effects.
In the words of international bipolar expert, Jim Phelps MD, “Lithium is like two different medications: low doses are pretty easy to manage and produce few side effects. High doses are tricky to manage, require close monitoring to stay safe, and can cause side effects which make people want to consider alternative treatments.”
This is something I learned the hard way. The day I was diagnosed as bipolar my psychiatrist lent me a copy of Kay Redfield Jamison’s autobiography, An Unquiet Mind.
It is a wonderful book and reading it answered a lot of questions for me. But it completely freaked me out about taking the “miracle” salt because Dr. Jamison describes having terrible side effect problems with reading and concentration.
Then I did something really dumb – went on an amateur website about psychotropic medication and read that taking it makes you fat, bald, and stupid. I never did any proper research, and I missed a really important passage in Dr. Jamison’s book about what happened WHEN THE PATIENT SWAPPED TO A LOWER DOSE!
So, I tried Depakote, Geodon, Neurontin, and a whole lot of other things – and guess what – they made me fat, bald and stupid. More to the point, they did NOT stabilize me.
Finally, at the point of last resort I tried it. WOW! Now I am stable, happy and healthy. And I have finally read the part in An Unquiet Mind where Dr. Jamison describes the benefits of being on a low dose. Duh!
Consumer Reports:
“If you take lithium, you are much less likely to have a relapse of bipolar disorder. It works as well as valproate, carbamazepine, or lamotrigine for preventing a relapse. But it seems to be better at preventing new symptoms of mania than at preventing new symptoms of depression.”
Summary of Lithium Pros and Cons
Lithium has the most research and evidence behind it and is particularly known as an anti manic. It is good for preventing suicide, but weak against depression.
Lamictal has evidence showing effectiveness against depression, but is not as effective against mania.
Zyprexa (olanzapine) is very effective, but is so strongly associated with weight gain, diabetes and other serious side effects that it rarely the preferred first choice.
Why is Lithium Still the Gold Standard?
Why is lithium still regarded as the first line treatment for bipolar symptoms?
The main reason is that it treats the broad range of bipolar symptoms more completely than any other medication. It is effective against both mania and depression, and it reduces the risk of suicide.
It also does well in stabilizing mood and slows down the frequency of cycling – which is why it is a good maintenance therapy. Plus, we have the most research on it, it is much cheaper than new medications, and it is arguably the most “natural” medication, being based on a simple and naturally occurring mineral salt.
CLINICAL UPDATE: Major Findings in Bipolar Disorder: “Findings suggest that the combination of lithium and lamotrigine may be particularly advantageous in long-term treatment.”
The Downside
Lithium does require more proactive management than other medications. The level in the blood must be kept within a very narrow range. Too little and it is possible to slip back into mania or depression – too much and side effects may become unpleasant or you may even risk death or serious health problems s from lithium toxicity.
Lithium Dosage Explained: Is 300 mg a Low Dose?
The common US brands are Eskalith, Eskalith CR and Lithobid. In Canada you will see Carbolith, Duralith and Lithane. Sometimes lithium meds come as simple generics are labelled with chemical names such as lithium carbonate or lithium citrate.
The form may be as a capsule, extended release tablet, or a liquid solution.
Dosing may be 2-3 or 3-4 times per day, depending on how much you need and whether or not you are using the extended release version.
Usually each tablet, capsule, or teaspoon of liquid contains 300 milligrams; but 150, 450, and 600 milligram variations are also available.

Exact doses and dosing schedules will be based on your blood test results, body mass, diet, symptoms, and individual response. The goal is to minimize the dose in order to minimize side effects while also ensuring you maintain a high enough and constant enough level of lithium in your blood to prevent mood swings.
Patty Duke, for example, takes her “little beige pills” twice a d your blood level is 0.7 mEq/L, then for your body, 300 mg is a perfect, effective dose—not necessarily “low.”
Lithium Side Effects: What’s Common vs. Serious
While lithium is highly effective, it is a medication that requires respect. Many patients are deterred by stories they hear online, but understanding the difference between “nuisance” side effects and “serious” risks can help you manage your treatment with confidence.
What Is the Biggest Side Effect of Lithium?
If you ask a group of patients, the answer is usually thirst and frequent urination. Because lithium is a salt, it forces your kidneys to work harder to maintain balance, a condition sometimes called “nephrogenic diabetes insipidus.” While it sounds scary, for most, it simply means carrying a water bottle everywhere and taking more trips to the bathroom.
“Lithium Belly”: Weight Gain & Bloating Explained
“Lithium belly” is a term patients often use to describe the bloating, gas, and weight gain associated with the drug.
- The Mechanism: Lithium can slow down your metabolism slightly and increase sugar cravings.
- Water Retention: Because it is a salt, your body may hold onto more water than usual.
- The Solution: We often recommend a “Bipolar Diet”—one low in processed sugars and high in hydration—to counteract these effects. In many cases, the weight gain is manageable if caught early through lifestyle changes.
Cognitive Slowing and “Fog”
Some users describe a “mental fog” or a feeling that they are “slower” at processing information. This is often a sign that the dose may be slightly too high. By working with your doctor to find the “lowest effective dose,” many patients find that this fog lifts, leaving them stable but sharp.
Thyroid and Kidney Effects
Long-term lithium use can affect the thyroid gland (leading to hypothyroidism) and, in rare cases, the kidneys. This is exactly why we perform regular lab work. Most thyroid issues caused by lithium are easily treated with a simple thyroid hormone supplement, allowing the patient to stay on their life-saving lithium.
What Happens If You Miss a Dose of Lithium?
Consistency is the foundation of lithium therapy. Because we are maintaining a very specific “therapeutic window” in your blood, skipping a pill can cause your levels to drop quickly.
Short-Term Effects
If you miss a single dose, you might not feel anything immediately. However, for those who are sensitive, a drop in levels can trigger a “rebound” of symptoms. You might feel irritable, shaky, or notice your racing thoughts returning within 24 to 48 hours.
What Not to Do: The Double-Dosing Trap
If you realize you missed a dose, never double up to “catch up.” Taking a double dose can push your blood levels into the toxic range (above 1.5 mEq/L). If it is almost time for your next dose, simply skip the missed one and get back on your regular schedule. If you are unsure, call your pharmacist or doctor.
Lithium Medication Patient Education
Up-to-date, accurate, and complete lithium patient education is proven to significantly enhance outcomes.
Medication compliance, symptom level, weight gain, and quality of life are all on-going challenges for people taking lithium.
Patient education has been demonstrated by research to improve all of these problems.
Lithium medication patient education may focus on any of the following:
1. Taking medication as directed.
2. Understanding risk factors for relapse.
3. Recognizing warning signs for relapse.
4. Managing stress.
5. Identifying supportive strategies.
In fact, education is emerging as one of the most successful psychological and social interventions for bipolar disorder.
As well as improving medication compliance and attitudes to lithium, education has been shown to reduce relapses and improve social and occupational functioning.
Drug companies who provide lithium medication routinely provide lithium medication patient education sheets along with the drugs. You have probably received one of these from your pharmacy.
Lithium Medication FAQ
1. Is lithium addictive?
No.

2. Does lithium cure bipolar?
No. It is an effective treatment, but it is not a cure. Someone who stops taking their lithium medication will probably relapse. . Think of it as a symptom management tool.
3. Will I ALWAYS have to have blood tests?
Yes. However these become needed far less frequently with time and today there is an innovative new test available that can be administered right there in the doctor’s office.
4. How should lithium be stored?
In a cool, dry, dark place, out of reach of children. Don’t keep your lithium medication in the refrigerator or in the bathroom.
5. Does lithium require a prescription?
Yes! It also requires careful monitoring from an expert clinician who is experienced in looking after patients on lithium medication! This is NOT one of those medications to buy over the Internet!
6. What are some good sources of further information?
A nice easy read that still has plenty of detail is the excellent booklet, by James W. Jefferson & John H. Greist Lithium and Bipolar Disorder: A Guide, Lithium Information Center, Madison Institute of Medicine, 2004, available from Amazon for just $5.95.
Reliable, trustworthy and unbiased information on lithium medication is available in lay terms from two very experienced doctors: Jim Phelps MD and world expert, Dr Manji.
WARNING – Only read the above links from Dr Phelps and Dr Manji if you want some GOOD NEWS for a change!
Final Thoughts: Your Journey with the “Miracle Salt”
Lithium is more than just a pill; for many, it is the difference between a life of chaos and a life of purpose. While the myths of being “bald, fat, and stupid” persist on the internet, the clinical reality is that lower, modern doses have made lithium more tolerable than ever before.
If you are struggling with the highs and lows of bipolar disorder, talk to your doctor about the “oldest” treatment on the shelf. It might just be the most modern solution for your brain.
References:
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2800957/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2990551/
- https://www.mdedge.com/psychiatry/article/82687/bipolar-disorder/lithium-bipolar-disorder-re-emerging-treatment-mood
- Rybakowski, J. K. (2018). Challenging the negative perception of lithium and optimizing its long-term administration. Frontiers in molecular neuroscience, 11, 349.
- Malhi, G. S., Gessler, D., & Outhred, T. (2017). The use of lithium for the treatment of bipolar disorder: recommendations from clinical practice guidelines. Journal of affective disorders, 217, 266-280.
- Cipriani, A., Hawton, K., Stockton, S., & Geddes, J. R. (2013). Lithium in the prevention of suicide in mood disorders: updated systematic review and meta-analysis. Bmj, 346, f3646.
- Bobes, J., Rejas, J., Garcia-Garcia, M., Rico-Villademoros, F., Garcıa-Portilla, M. P., Fernández, I., … & EIRE Study Group. (2003). Weight gain in patients with schizophrenia treated with risperidone, olanzapine, quetiapine or haloperidol: results of the EIRE study. Schizophrenia Research, 62(1-2), 77-88.

Related Posts





Subscribe to Our Newsletter
Get mental health tips, updates, and resources delivered to your inbox.
MORE from Author
Read More In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure…
In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure…- We all have "up" days and "down" days. Perhaps you feel energized after a promotion or sluggish on a rainy…


 To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,…
To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,… To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…
To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…


Are you looking for a Therapist?
Connect with qualified mental health professionals who understand
bipolar disorder, mood changes, and emotional challenges.
Private • Supportive • Confidential