What Is the Best Therapy for Bipolar Disorder? (2026 Guide)

Medically reviewed by Carolina Estevez, Psy.D Updated Date: April 15, 2026

If you or a loved one has recently received a diagnosis, you likely have one pressing question: What is the best therapy for bipolar disorder? Living with bipolar disorder can feel like navigating an unpredictable emotional ocean, where waves of high-energy mania crash into deep troughs of depression. The search for the most effective treatment for bipolar disorder is not just about stopping the swings; it is about reclaiming your life.
As of 2026, the clinical consensus is clear: the “best” treatment is rarely a single pill or a lone therapy session. Instead, it is a personalized, multi-pronged approach known as the combined treatment model. By pairing modern pharmacological interventions with specialized psychotherapy, individuals can achieve long-term stability that was once thought impossible.
In this pillar guide, we will explore the treatment recommendations for bipolar disorder based on the latest 2026 research, compare the needs of Bipolar 1 vs. Bipolar 2, and dive deep into the specific therapy modalities that are proven to work. Whether you are looking for clinical reassurance or practical daily habits, this guide serves as your roadmap to stability.
What Causes Bipolar Disorder?
Understanding what causes bipolar disorder is the first step in de-stigmatizing the condition. It is not a character flaw or a simple “moodiness.” Rather, it is a complex biological condition.

The Biological Blueprint
- Genetic Factors: Bipolar disorder is highly heritable. Recent 2026 genomic studies, such as the discovery of the AKAP11 gene as a major risk factor, have highlighted how certain genetic variations influence brain signaling.
- Neurochemistry: The disorder is linked to the dysregulation of neurotransmitters—the brain’s chemical messengers—like dopamine, serotonin, and norepinephrine. These chemicals govern energy, reward, and mood.
- Brain Structure: Advanced neuroimaging now shows structural differences in the areas of the brain responsible for emotion regulation, such as the prefrontal cortex and the amygdala.
The Environmental “Match”
While biology provides the dry wood, the environment is often the spark. Stressful life events, trauma, or severe disruptions to sleep can “kindle” an episode. This is why what helps with bipolar disorder must include both biological management (medication) and environmental management (therapy and lifestyle).
Bipolar 1 vs. Bipolar 2: Treatment Differences Explained
While they share a name, Bipolar 1 and 2 treatment plans often look quite different because the primary symptoms vary in intensity and nature.
Bipolar 1: Managing Mania
Bipolar 1 is defined by at least one manic episode. Mania involves extreme euphoria, racing thoughts, and sometimes a break from reality (psychosis).
- Treatment Focus: The priority is often preventing acute mania. Most effective treatment for bipolar type 1 usually involves more intensive use of mood stabilizers or antipsychotics to “cap” the highs before they lead to hospitalization.
Bipolar 2: Targeting Depression
Bipolar 2 involves “hypomania”—a less severe high that doesn’t cause a total break from functioning—but is characterized by much more frequent and debilitating depressive episodes.
- Bipolar 2 Treatment Options: Because the “lows” are the dominant feature, therapy often focuses heavily on depression management and anxiety reduction. Best treatment for bipolar 2 frequently utilizes medications like Lamotrigine or Quetiapine, which have strong antidepressant properties without the high risk of “switching” the patient into mania.
What Is the Most Effective Treatment for Bipolar Disorder?
According to bipolar disorder treatment scholarly articles published in 2025 and 2026, the “Gold Standard” is the Integrated Care Model.
The Gold Standard Rule: Medication provides the biological floor (stopping the fall into depression) and the ceiling (stopping the rise into mania), while psychotherapy builds the architecture of the room (coping skills and routine).
Why One Isn’t Enough
Medication alone may stop a manic episode, but it cannot teach a person how to repair a relationship damaged during that episode. Conversely, therapy alone is rarely enough to correct the profound chemical shifts of a severe manic or depressive state.
Treatment recommendations for bipolar disorder now emphasize a team-based approach involving a psychiatrist for medication management and a licensed therapist specializing in bipolar-specific modalities.
Best Therapy Modalities for Bipolar Disorder

Choosing the right talk therapy is critical. Not all counseling is created equal when it comes to mood disorders. Here are the best therapy modalities for bipolar disorder currently in use.
5.1 Cognitive Behavioral Therapy (CBT)
Cognitive behavioral therapy for bipolar disorder is one of the most researched interventions. It focuses on the relationship between thoughts, feelings, and behaviors.
- Core Focus: Identifying “automatic” negative thoughts that fuel depression and “over-optimistic” thoughts that fuel mania.
- The Skill: CBT teaches patients to recognize their “Relapse Signature”—the unique set of symptoms (like sleeping less or talking faster) that appear just before a mood swing.
5.2 Interpersonal and Social Rhythm Therapy (IPSRT)
If you ask a specialist what helps with bipolar disorder, they will likely point to IPSRT. This therapy is based on the idea that bipolar symptoms are triggered by disruptions in the body’s internal clock (circadian rhythms).
- Core Focus: Stabilizing daily routines. Patients track their “Social Rhythm Metric,” aiming for consistent times for waking, eating, and social interaction.
- The Goal: By keeping the body’s clock stable, you make it much harder for a mood episode to take root.
5.3 Family-Focused Therapy (FFT)
Bipolar disorder doesn’t just happen to an individual; it happens to a family. Family-focused therapy for bipolar disorder involves loved ones in the healing process.
- Core Focus: Communication training and psychoeducation.
- The Skill: Families learn what not to say to someone with bipolar and how to spot warning signs without becoming “the mood police.” This reduces the high-stress home environments that often trigger relapses.
5.4 Other Supportive Therapies
- Psychoeducation: This is the foundation of all treatment. It involves learning the “mechanics” of the illness so you can become an expert in your own care.
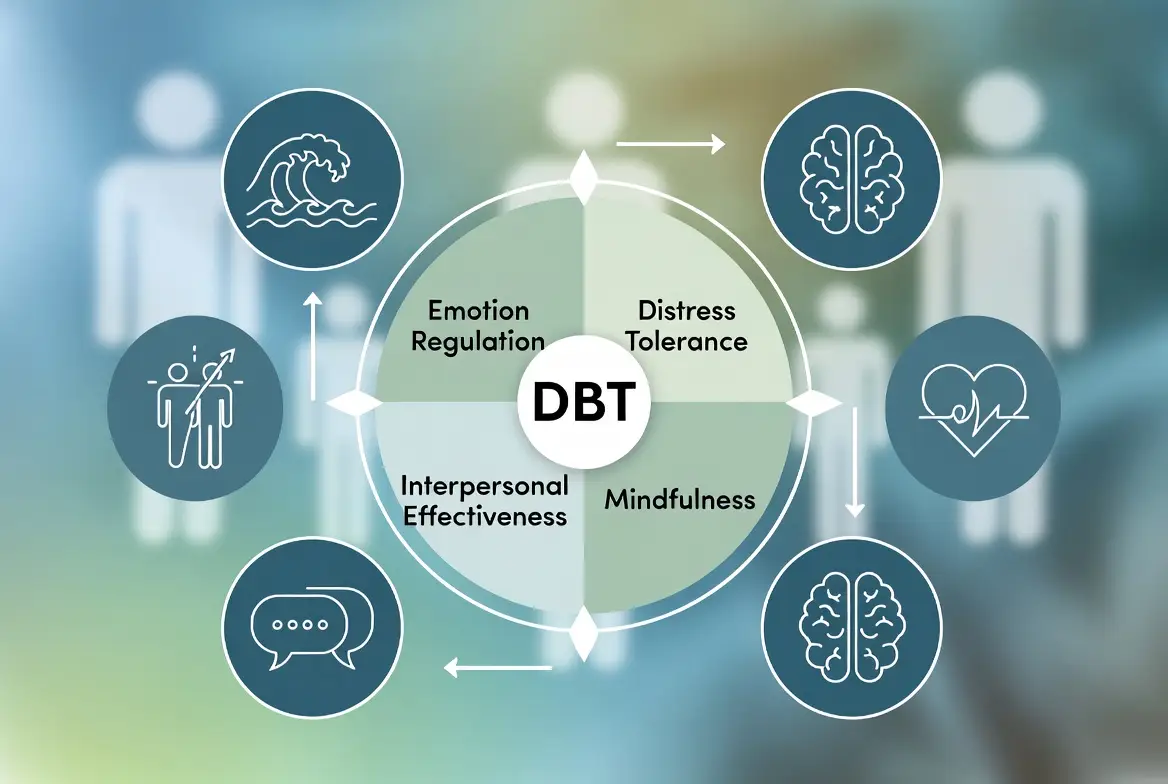
- Dialectical Behavior Therapy (DBT): Excellent for those who struggle with intense irritability or rapid mood shifts, focusing on mindfulness and distress tolerance.
Best Therapy for Bipolar Anxiety & Mood Swings
Anxiety is an often-overlooked companion to bipolar disorder, affecting up to 50% of patients. The best treatment for bipolar anxiety usually involves a careful balance.
- The Challenge: Traditional anti-anxiety medications (like SSRIs) can sometimes trigger mania in bipolar patients.
- The Therapy Solution: CBT and mindfulness-based therapies are the first-line recommendations for managing anxiety without destabilizing the mood.
- The Sleep Foundation: Sleep is the single most important non-medical treatment. Experts often ask, “How many hours should bipolar sleep?” The consensus is 7–9 hours of consistent, high-quality sleep. Even one “all-nighter” can be enough to trigger a manic episode for some.
Medications Used for Bipolar Disorder

Medication is the cornerstone that makes therapy possible. While only a doctor can prescribe, knowing what medication is used for bipolar disorder helps you advocate for yourself.
1. Mood Stabilizers
- Lithium: The oldest and still the “Gold Standard.” It is uniquely effective at reducing suicide risk and preventing mania.
- Anticonvulsants: Drugs like Valproate (Depakote) or Lamotrigine (Lamictal) are used to level out the “waves.” Lamotrigine is particularly favored for the best therapy for bipolar 2 due to its antidepressant properties.
2. Atypical Antipsychotics
Modern medications like Quetiapine (Seroquel), Lurasidone (Latuda), and Cariprazine (Vraylar) are now frequently used as first-line treatments for both acute episodes and long-term maintenance.
3. The Antidepressant Risk
Antidepressants are used cautiously. If used without a mood stabilizer, they can cause “switching” into mania or rapid cycling.
Medical Disclaimer: The information above is for educational purposes and does not constitute medical advice. Always consult with a qualified psychiatrist or medical professional before starting or stopping any medication.
Lifestyle, Diet & Daily Habits That Support Treatment
What you do between doctor visits is just as important as the visits themselves. What worsens bipolar? Stress, substance use, and irregular habits.
Nutrition and Diet
When people ask, “What foods should someone with bipolar disorder avoid?” the answer isn’t about one specific “poison” but rather about blood sugar and inflammatory balance.
- Avoid: Excessive caffeine (triggers mania) and alcohol (a depressant that interferes with meds).
- Focus on: Omega-3 fatty acids (found in fish or supplements), complex carbohydrates for stable energy, and staying hydrated—especially if taking Lithium.
The Power of Routine
Because the bipolar brain is sensitive to change, a rigid routine is a superpower. Regular exercise, daily sunlight exposure, and a strict “no-screens” policy before bed help maintain the social rhythms discussed in IPSRT.
Can You Live a Normal Life With Bipolar Disorder?
The most common fear after a diagnosis is, “Will I ever be normal with bipolar?” The answer is a resounding yes. While there is currently no cure, bipolar disorder is highly manageable. “Normal” in the context of bipolar means having the tools to catch a swing before it becomes a crisis. With adherence to the most effective treatment for bipolar, many people go years—or even decades—without a major episode.
Lifespan and Quality of Life
You may have read statistics about the average lifespan of a person with bipolar disorder being shorter. It is important to know that these statistics are largely driven by untreated cases (suicide and cardiovascular issues). With modern treatment, regular exercise, and consistent medical care, those risks are drastically reduced. Success isn’t the absence of a disorder; it’s the mastery of it.
What Not to Say to Someone With Bipolar Disorder
Supportive communication is a part of treatment. Stigma is one of the biggest factors in what worsens bipolar disorder because it prevents people from seeking help.
- Avoid: “Are you manic right now?” (This invalidates real emotions).
- Avoid: “Everyone has mood swings.” (This minimizes a clinical condition).
- Instead, try: “I’ve noticed you’re having a hard time. How can I best support you today?” or “I’m here for you, regardless of your mood.”
Treatment Plans & PDFs: What They Include
When you start therapy, you might receive a treatment plan for bipolar disorder pdf or a workbook. These aren’t just paperwork; they are your survival guide.
Common Elements:
- Mood Charting: A daily log to find patterns.
- Trigger List: A list of things that “start” the fire (e.g., travel, conflict).
- Emergency Contact List: Who to call when you lose the ability to judge your own mood.
- Medication Tracker: To ensure consistency and note side effects.
The Neurobiology of Mood: Why Your Brain Needs Targeted Therapy

To truly understand what helps with bipolar disorder, we must look at the biological “machinery” that therapy is trying to repair. Scholarly research indicates that bipolar disorder is a condition of neuroplasticity and connectivity.
The “Broken Thermostat” Analogy
In a neurotypical brain, the prefrontal cortex (the logical center) acts as a thermostat for the amygdala (the emotional center). When the amygdala gets too hot (mania) or too cold (depression), the prefrontal cortex sends signals to bring it back to a baseline. In a bipolar brain, this connection is frayed.
- During Mania: The logical center is essentially “off-line,” allowing the emotional center to run without a governor.
- During Depression: The logical center becomes hypercritical, trapping the brain in a loop of negative rumination.
How Therapy Changes Brain Structure
This is where the best therapy modalities for bipolar disorder prove their worth. Studies using fMRI technology show that consistent Cognitive Behavioral Therapy (CBT) can actually strengthen the physical neural pathways between these two regions. By practicing “top-down” regulation techniques, you are physically re-wiring your brain to regain control over your moods.
Deep Dive: Advanced Techniques in Bipolar Psychotherapy
We previously touched on CBT and IPSRT, but let’s look at the specific, high-level techniques used within these sessions to manage bipolar mood swings.
5.5 Dialectical Behavior Therapy (DBT) for Emotional Storms
While CBT manages thoughts, DBT is often the best therapy for bipolar patients who struggle with intense, rapid-fire irritability or “mixed features.”
- Distress Tolerance: This isn’t about fixing the mood; it’s about surviving it. Techniques like TIPP (Temperature, Intense exercise, Paced breathing, and Paired muscle relaxation) help lower the physiological “heat” of a manic or mixed episode.
- Mindfulness of “Wise Mind”: Patients learn to find the middle ground between their “Emotional Mind” (the bipolar surge) and their “Rational Mind.”
5.6 Metacognitive Therapy (MCT)
A newer entrant in bipolar disorder treatment scholarly articles, MCT doesn’t just look at what you think, but how you think.
- Detached Mindfulness: Instead of engaging with a depressive thought like “I am worthless,” you observe the thought as a passing cloud. This prevents “rumination,” which is the primary fuel for a depressive relapse.
The Pharmacology of Stability: A 2026 Deep Dive
Medication is often the most stressful part of the journey. Understanding the most effective treatment for bipolar disorder requires knowing exactly what these drugs do to your brain.
Mood Stabilizers: The Foundation
- Lithium (The Gold Standard): Lithium works by modulating the “G-protein” signaling in the brain. It doesn’t just suppress mania; it actually protects neurons from the stress of a mood episode. Because it requires regular blood testing to monitor kidney and thyroid function, it is the ultimate example of recommended treatment for bipolar disorder, requiring a partnership with your doctor.
- Lamotrigine (The Depression Shield): In bipolar 2 treatment options, Lamotrigine is a superstar. It blocks voltage-sensitive sodium channels, essentially preventing the brain from “slowing down” too much into a depressive state.
Atypical Antipsychotics: The Modern “Swiss Army Knife”
In 2026, drugs like Lurasidone and Cariprazine are the most frequently prescribed for bipolar depression. Unlike older antipsychotics, these target specific dopamine receptors (D3) that influence motivation and reward, helping to lift the “anhedonia” (inability to feel pleasure) that characterizes bipolar lows.
What Worsens Bipolar? The “Kindling Effect”

To stay stable, you must understand the Kindling Effect. This theory suggests that each untreated mood episode makes the brain more sensitive to future episodes.
Factors That “Kindle” the Fire:
- Sleep Deprivation: As mentioned, even one night of missed sleep can trigger mania. This is because sleep loss causes a massive spike in dopamine, which a bipolar brain cannot regulate.
- Caffeine and Stimulants: These mimic the beginning of a manic episode, tricking the brain into “switching.”
- Interpersonal Conflict: High-stress relationships are a leading cause of relapse. This is why family-focused therapy for bipolar disorder is so critical—it cools the environment so the brain can heal.
- Alcohol and Substance Use: Substance use is often “self-medication,” but it destabilizes the very receptors that your actual medication is trying to fix.
The 2026 Lifestyle Protocol: “Social Rhythm Tracking”
If you want to know what helps with bipolar disorder in a practical sense, it is the Social Rhythm Metric (SRM). This is a tool often found in a psychotherapy for bipolar disorder pdf.
The 5 Anchors of Stability:
- Out of Bed: Must be within the same 30-minute window every day, including weekends.
- First Contact: The first time you interact with another human (even via phone). This resets your social clock.
- Start of Activity: Beginning your work, school, or primary daily task.
- Dinner: Your body’s metabolic clock is tied to your mood clock.
- Lights Out: Not just when you get in bed, but when the screens go off.
Can You Be Normal? Redefining Recovery
The question “Will I ever be normal with bipolar?” often stems from the fear of being “flat” or “medicated into a zombie.”
Functional vs. Symptomatic Recovery
- Symptomatic Recovery means you have no symptoms. This is a great goal, but it isn’t the only one.
- Functional Recovery means you are living the life you want. You might still have “echoes” of the disorder—a few days of low energy or a few nights of restless sleep—but they no longer have the power to destroy your career or your family.
In 2026, the average lifespan of a person with bipolar disorder is being redefined by this focus on “whole-body health.” By managing blood pressure, inflammation, and metabolic health alongside mood, the gap between bipolar and neurotypical lifespans is closing rapidly.
Frequently Asked Questions
What is the best therapy for bipolar disorder?
The most effective treatment for bipolar disorder is a combination of Lithium or mood stabilizers and Interpersonal and Social Rhythm Therapy (IPSRT) or CBT.
What helps with bipolar disorder?
Consistency is key. Medication adherence, 8 hours of sleep, avoiding alcohol, and having a strong support system are the most helpful interventions.
What medication is used for bipolar disorder?
Standard treatments include mood stabilizers (Lithium, Lamotrigine) and atypical antipsychotics (Quetiapine, Aripiprazole).
What worsens bipolar disorder?
Sleep deprivation, high stress, illicit drug use, and “monotherapy” antidepressants (without a mood stabilizer) are the primary triggers for relapse.
Will I ever be normal with bipolar?
Yes. With modern treatment, most people live full, successful lives. Stability is achieved through a “partnership” between you and your clinical team.
What medication is used for bipolar disorder most often in 2026?
While Lithium remains the gold standard, atypical antipsychotics like Vraylar (Cariprazine) and Latuda (Lurasidone) are the most common first-line treatments for the depressive phases of Bipolar 1 and 2.
What foods should someone with bipolar disorder avoid?
There is no “bipolar diet,” but scholarly research suggests avoiding high-sugar foods that cause insulin spikes, as these can trigger irritability and “mixed” symptoms. A Mediterranean-style diet high in healthy fats (Omega-3s) is currently the most recommended treatment for bipolar nutritional support.
How many hours should a bipolar person sleep?
Consistency is more important than quantity. Most specialists recommend 8 solid hours. Getting 10 hours one night and 5 the next is more dangerous than getting 7 hours every single night at the exact same time.
Conclusion
Living with bipolar disorder is a marathon, not a sprint. While there is no “one-size-fits-all” answer to what is the best therapy for bipolar disorder, the evidence points toward the integrated care of medication and specialized psychotherapy.
If you are struggling today, your next step is to find a provider who understands the treatment recommendations for bipolar disorder and can help you build a treatment plan for bipolar disorder pdf. Remember, the goal isn’t just to stop being “bipolar”—it’s to start being yourself again.
Authoritative References
1. National Institute of Mental Health (NIMH)
2. American Psychiatric Association (APA)
3. Mayo Clinic: Bipolar Diagnosis & Treatment
4. Depression and Bipolar Support Alliance (DBSA)
5. National Institute for Health and Care Excellence (NICE)
SEO Title Tag (58 Characters)
Best Therapy for Bipolar Disorder: Evidence-Based Care Guide
Meta Description (152 Characters)
Discover the most effective treatment for bipolar disorder. Explore scholarly research on CBT, IPSRT, and medication protocols for long-term stability.
Related Posts

Subscribe to Our Newsletter
Get mental health tips, updates, and resources delivered to your inbox.
MORE from Author
Read More In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure…
In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure… We all have "up" days and "down" days. Perhaps you feel energized after a promotion or sluggish on a rainy…
We all have "up" days and "down" days. Perhaps you feel energized after a promotion or sluggish on a rainy…
 To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,…
To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,… To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…
To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…
Are you looking for a Therapist?
Connect with qualified mental health professionals who understand
bipolar disorder, mood changes, and emotional challenges.
Private • Supportive • Confidential