Premenstrual Exacerbation: Why Symptoms Worsen Before Your Period and How to Treat Them

Medically reviewed by Laura Athey Updated Date: March 25, 2026
In my practice as a clinical psychologist, I often sit with patients who feel as though they are “failing” at their recovery for one week out of every month. They describe a baffling phenomenon: their depression, which seemed manageable on Tuesday, becomes agonizing by Friday.
Their anxiety, once quieted by therapy, suddenly spikes into nocturnal panic. For many women and individuals assigned female at birth (AFAB), this isn’t just “bad PMS.” It is premenstrual exacerbation (PME).
What is premenstrual exacerbation? Simply put, it occurs when an existing mental health condition—such as MDD, GAD, ADHD, or bipolar disorder—significantly worsens during the luteal phase (the days leading up to menstruation).
Unlike Premenstrual Dysphoric Disorder (PMDD), where symptoms disappear entirely after the period starts, PME involves a baseline of symptoms that exist all month but are amplified to an unbearable degree by shifting hormones. This distinction is vital because treating PME requires a different clinical strategy than treating standard PMS.
What Is Premenstrual Exacerbation (PME)?
To understand the PME premenstrual exacerbation definition, we must look at the word “exacerbation” itself. It means to make a problem or a bad situation worse.
In the context of reproductive psychology, PME is the clinical term for the cyclical worsening of a chronic psychiatric or physical condition during the premenstrual window.
In my practice, I often observe that patients with PME feel gaslit by the term “mood swings.” PME isn’t a swing; it’s an intensification. If you have a “volume knob” for your anxiety, PME is the hand that cranks that knob from a 3 to a 9 every twenty-eight days.
Crucially, for a diagnosis of PME, the symptoms must be present throughout the entire cycle but become significantly more severe in the week or two before menses.
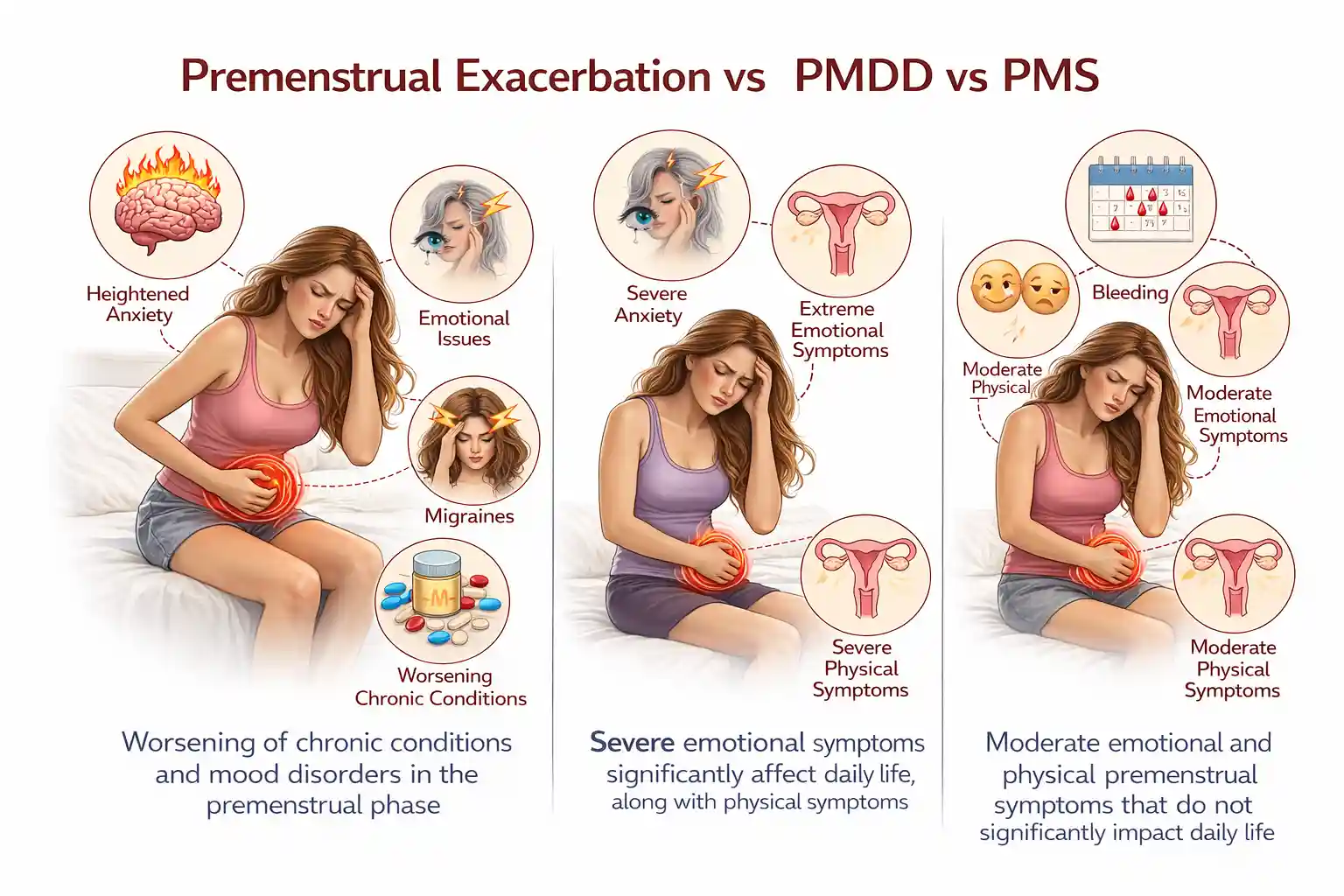
Premenstrual Exacerbation vs PMDD vs PMS
One of the most frequent questions I receive is about the difference between PMS and PMDD and how both differ from PME. Misdiagnosis is rampant in this area, which is heartbreaking because the treatment for one may not work for the other.
| Condition | Core Feature | Symptom Timing | Baseline Symptoms? |
| PMS | Mild physical/emotional discomfort. | 3–5 days before the period. | No. |
| PMDD | Severe, debilitating mood disorder. | Luteal phase only. | No symptoms during the follicular phase. |
| PME | Existing disorder worsens. | Luteal phase. | Yes, symptoms persist all month. |
Premenstrual exacerbation vs. PMDD is the trickiest distinction. In PMDD, the person is essentially “asymptomatic” (free of symptoms) for at least a week after their period ends.
In PME, the person still struggles with their primary diagnosis (like OCD or depression) during that week, but they feel more equipped to handle it than they do during the premenstrual “dip.”
Premenstrual Exacerbation Symptoms
When we discuss premenstrual exacerbation symptoms, we are really discussing the “shadow version” of your primary diagnosis. Because PME is an amplifier, the symptoms look like your underlying condition, only harder to ignore.
Emotional and Cognitive Symptoms
- Irritability and “Period Rage”: A sudden inability to tolerate minor stressors that would normally be handled with ease.
- Anxiety Spikes: An increase in physical tremors, racing thoughts, or the feeling of impending doom.
- Emotional Sensitivity: Taking feedback more personally or feeling a profound sense of rejection (rejection-sensitive dysphoria).
Behavioral and Physical Symptoms
- Social Withdrawal: A common social withdrawal premenstrual symptom where the person feels they must isolate to “protect” others from their mood or to protect themselves from sensory overload.
- Executive Function Collapse: Especially in those with ADHD, a total inability to start tasks or manage time.
- Fatigue: A “bone-tired” exhaustion that sleep does not fix.
What Causes Premenstrual Exacerbation?
This is the “Main Topic” of our exploration, and it is where the biology of the endocrine system meets the psychology of the mind. To understand why PME happens, we have to look at the brain’s sensitivity to hormonal flux.
The Hormonal Trigger: Estrogen and Progesterone
During the luteal phase (after ovulation), estrogen levels drop sharply, and progesterone rises and then falls. For most people, this is a minor shift. But for those with PME, the brain is hypersensitive to these fluctuations.
It isn’t that people with PME have “abnormal” hormone levels—blood tests often show their levels are perfectly within the “normal” range.
Rather, their neurotransmitters are more sensitive to the change in those levels. Think of it like a thermostat: in a typical brain, the thermostat adjusts smoothly to a 5-degree drop in temperature. In a PME brain, that 5-degree drop triggers a “system error.”
Neurotransmitter Interaction: The “Why” Behind the Biology
The primary reason mental health symptoms worsen is the relationship between hormones and neurotransmitters like serotonin, GABA, and dopamine.
- Serotonin and Estrogen: Estrogen helps the brain produce and maintain serotonin (the “feel-good” and “calm” chemical). When estrogen drops premenstrually, serotonin levels often drop with it. If you already have premenstrual exacerbation of depression, this drop takes your already low serotonin and pushes it into the “danger zone,” leading to hopelessness or suicidal ideation.
- GABA and Allopregnanolone: Progesterone breaks down into a neurosteroid called allopregnanolone, which usually acts on GABA receptors to calm the brain (like a natural Valium). However, in some individuals, the brain has a paradoxical reaction to this chemical, leading to agitation and anxiety instead of calm.
- Dopamine and ADHD: Estrogen also modulates dopamine, the chemical responsible for focus and reward. When estrogen is low, dopamine signaling becomes less efficient. This is why premenstrual exacerbation of ADHD is so prevalent—the brain’s “operating system” literally loses its power source for a few days a month.
In my practice, I have found that sleep hygiene is the “canary in the coal mine” for PME. Progesterone increases body temperature, which can disrupt REM sleep.
For a patient with an existing anxiety disorder, one night of “hormonal insomnia” can completely erode their executive function the next day, making them far more vulnerable to a panic attack.
I often advise patients that while we cannot stop the hormone drop, we can mitigate the exacerbation by aggressively protecting sleep—using cooling blankets or strict bedtime rituals—specifically during the luteal week.
The Clinical Reality: A Story of “Mina”
I remember a patient, “Mina,” who came to me for what she thought was “failing” her treatment for Generalized Anxiety Disorder (GAD). She had been in therapy for a year and was doing well, but every few weeks, she would call me in a state of total crisis, convinced her husband was going to leave her and she was going to lose her job.
When we looked at her Calendar of Premenstrual Experiences (COPE), the pattern was undeniable. Her “crisis” always occurred 4 days before her period. Mina didn’t have PMDD—she had anxiety every day—but her PME turned her manageable worries into a perceived catastrophe.
We utilized a specific therapeutic intervention: CBT-based cycle mapping. Once Mina understood that her “thought spirals” were being amplified by her estrogen drop, she gained a sense of neuroplasticity.
She learned to tell herself, “This thought feels true, but my brain is currently under-resourced due to my cycle.” This “clinical distancing” prevented her from making impulsive life changes during her PME week and allowed her to stay on track with her long-term recovery.
Premenstrual Exacerbation of Depression and Anxiety
In my practice, premenstrual exacerbation of depression is one of the most common reasons patients seek a medication “top-up.” If you already live with major depressive disorder, the luteal phase can feel like falling into a dark well you had just spent three weeks climbing out of.
The biological “why” is tied to the drop in estrogen, which acts as a natural serotonin booster. When that booster is withdrawn, the baseline depression isn’t just present—it is unmasked and intensified.
Patients often report that their “inner critic” becomes much louder, and feelings of worthlessness that they usually manage with executive function become overwhelming.
Similarly, premenstrual exacerbation of anxiety often manifests as a physical “revving” of the nervous system. Because progesterone metabolites affect GABA receptors (the brain’s natural brakes), a shift in these hormones can lead to:
- Panic Attack Frequency: Patients who usually have one panic attack a month might have three in a single weekend.
- Intrusive Thoughts: The “sticky” nature of anxious thoughts becomes harder to shake, leading to loops of worry that interfere with sleep and productivity.
PME in Neurodivergence: ADHD, Autism, and OCD
The intersection of hormones and neurodivergence is a rapidly growing field in reproductive psychiatry. I often observe that my neurodivergent patients feel “more autistic” or “more ADHD” during their premenstrual week.
- Premenstrual Exacerbation of ADHD: Estrogen is a dopamine agonist. When it drops, your ADHD medication (like Adderall or Ritalin) may actually feel less effective. Patients report a total “brain fog,” increased impulsivity, and a collapse of their organizational systems.
- Premenstrual Exacerbation Autism: For those on the spectrum, the drop in estrogen often leads to a significantly lower threshold for sensory input. Meltdowns or shutdowns become more frequent because the brain’s ability to “filter” noise, light, or touch is chemically compromised.
- Premenstrual Exacerbation OCD: Research shows that premenstrual exacerbation of OCD is remarkably common; the drop in serotonin makes obsessions “stickier” and compulsions feel more urgent as a way to regain a sense of safety during a turbulent hormonal time.
How Do You Know If You Have PME?
Diagnosis is the first step toward relief. Because PME is often hidden behind a primary diagnosis, we use specific tools to “tease out” the hormonal influence.
Using the Calendar of Premenstrual Experiences (COPE)
The Calendar of Premenstrual Experiences (COPE) is the gold standard for tracking. Unlike a simple period tracker, the COPE asks you to rate the severity of specific symptoms (anxiety, fatigue, irritability) on a scale of 1–4 every single day for at least two cycles.
How to read your data:
- If your scores are a 1 (mild) all month but jump to a 4 (severe) before your period, you likely have PMDD.
- If your scores are a 2 (moderate) all month but jump to a 4 (severe) before your period, you likely have PME.
Premenstrual Exacerbation Test and ICD-10
While there isn’t a blood “test” for PME, a clinical interview combined with two months of tracking is considered diagnostic.
In medical records, premenstrual exacerbation ICD-10 coding usually falls under the primary diagnosis (e.g., F33.1 for recurrent depressive disorder) with a secondary note regarding the premenstrual tension (N94.3).
Treatment for Premenstrual Exacerbation
Treating PME is different from treating PMDD. In PMDD, we might only treat the patient during the “luteal phase.” In PME, we must optimize the treatment for the underlying condition first.
Medication for Premenstrual Exacerbation
- Luteal Phase Dosing: Some psychiatrists recommend a “boost” in medication (e.g., increasing an SSRI or ADHD stimulant) only during the 7–10 days before the period.
- Hormonal Contraceptives: Birth control that suppresses ovulation can “level the playing field” by preventing the sharp drops in estrogen and progesterone that trigger the exacerbation.
- Mood Stabilizers: For premenstrual exacerbation of bipolar disorder, ensuring that lithium or lamotrigine levels are optimized is the first line of defense to prevent a cyclical relapse into mania or depression.
Lifestyle and Therapeutic Interventions
- CBT and DBT: Dialectical Behavior Therapy (DBT) is particularly effective for PME. It teaches “distress tolerance” skills that help you survive the “storm week” without blowing up your life or relationships.
- Anti-Inflammatory Nutrition: Reducing caffeine and sugar during the luteal phase can help stabilize the blood sugar spikes that often mimic or worsen anxiety.
Frequently Asked Questions
Difference Between PME and PMDD
The primary difference is the presence of baseline symptoms. PME is the worsening of an existing disorder (like depression) that is present all month. PMDD is a standalone disorder where symptoms only exist in the week before a period and disappear entirely afterward.
Medication for Premenstrual Exacerbation
Treatment often involves “luteal phase boosting,” where the dose of an existing antidepressant or stimulant is slightly increased during the premenstrual week, or using hormonal birth control to stop the ovulation cycle.
PME and Menopause
Does PME stop after menopause? Generally, yes. Once the cyclical fluctuations of estrogen and progesterone cease, the “trigger” for the exacerbation is removed. However, the underlying disorder (like ADHD or anxiety) will still require management.
Duration of PME Symptoms
PME typically lasts for the duration of the luteal phase, which is 5 to 14 days. Symptoms usually begin to lift within 24–48 hours of the period starting, as estrogen levels begin their upward climb again.
Premenstrual Exacerbation of Bipolar Disorder
PME is highly prevalent in bipolar disorder, often causing “ultra-rapid cycling.” It is vital for patients to track their cycles, as the premenstrual drop can be a significant trigger for a depressive or mixed episode.
Conclusion
Living with premenstrual exacerbation can feel like a monthly betrayal by your own body. However, once you move from “I’m losing my mind” to “My brain is experiencing a cyclical neurotransmitter dip,” everything changes.
By mapping your cycle and working with a provider who understands reproductive psychiatry, you can stop the “stop-start” cycle of your recovery. You are not a different person for one week a month—you are a person who deserves a little extra support and grace during that time.
Authoritative References
- International Association for Premenstrual Disorders (IAPMD)
- American Psychiatric Association (APA) – PMDD and PME
- National Institutes of Health (NIH) – Hormonal Mood Disorders
- Massachusetts General Hospital (MGH) Center for Women’s Mental Health
Related Posts






Subscribe to Our Newsletter
Get mental health tips, updates, and resources delivered to your inbox.
MORE from Author
Read More In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure…
In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure… We all have "up" days and "down" days. Perhaps you feel energized after a promotion or sluggish on a rainy…
We all have "up" days and "down" days. Perhaps you feel energized after a promotion or sluggish on a rainy…
 To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,…
To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,… To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…
To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…
Are you looking for a Therapist?
Connect with qualified mental health professionals who understand
bipolar disorder, mood changes, and emotional challenges.
Private • Supportive • Confidential