Valproate: A Comprehensive Guide to Uses, Mechanisms, and Patient Safety

Medically reviewed by Laura Athey Updated Date: May 1, 2026

In my practice as a clinical psychologist, I often work with individuals who are navigating the complexities of chronic mood instability or neurological conditions.
When a psychiatrist or neurologist introduces valproate—often known by the brand names Depakote or Epilim—the conversation usually centers on its reputation as a “workhorse” medication.
It is a broad-spectrum tool, remarkably effective for everything from acute manic episodes in bipolar disorder to complex seizure patterns in epilepsy and the prevention of debilitating migraines.
However, for many of my patients, the initial relief of finding a medication that works is quickly met with questions about long-term safety. “What exactly is this doing to my brain?” or “How will this affect my physical health?” are questions I hear weekly.
Understanding what valproate is and how to manage its physiological “footprint” is the first step toward a successful, sustainable treatment journey.
Valproate and Sodium Valproate
To understand this medication, we must first clarify the terminology, as the names can be a source of confusion. The generic name usually refers to valproate sodium, valproic acid, or divalproex sodium. While they are chemically slightly different, they all deliver the same active valproate ion to your system.
Chemical Forms and Delivery
- Sodium valproate: The salt form is most commonly used in immediate-release and some liquid formulations.
- Valproic Acid: The acid form of the medication.
- Divalproex Sodium (Depakote): A coordinated compound of the two above, often used in delayed-release tablets to reduce stomach upset.
Primary Indications
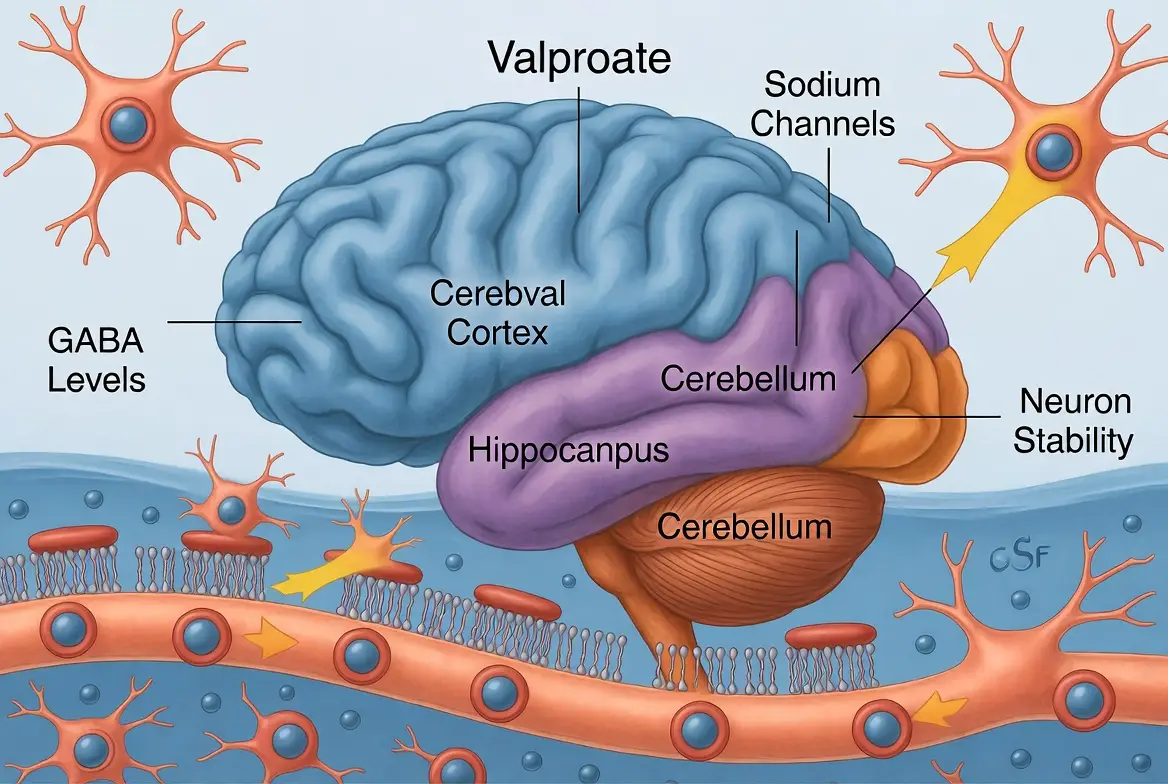
Valproate has become one of the most clinically versatile neuropsychiatric medications because it acts on multiple pathways in the central nervous system.
It increases the availability of gamma-aminobutyric acid (GABA), one of the brain’s primary calming neurotransmitters, while also helping regulate excessive neuronal firing. This dual mechanism explains why it is useful across several seemingly different conditions.
Bipolar Disorder: It is a cornerstone treatment for acute mania and long-term mood stabilization. It is particularly effective for mixed episodes, where symptoms of agitation, racing thoughts, and elevated energy occur alongside depression, hopelessness, or irritability.
In many patients, valproate can reduce impulsivity, aggression, sleep disruption, and rapid mood cycling.
Epilepsy: As a broad-spectrum anticonvulsant, it is widely used for generalized seizures, focal (partial) seizures, absence seizures, and certain difficult-to-control seizure syndromes. Because it targets multiple seizure types, it is often chosen when patients have complex or mixed seizure presentations.
Migraine Prophylaxis: It is frequently prescribed to reduce the frequency, severity, and duration of chronic migraines in adults. For individuals with recurrent disabling headaches, regular preventive therapy may significantly improve daily functioning and quality of life.
Valproate pronunciation is typically val-pro-ate. Whether it is administered as valproate syrup for pediatric patients, delayed-release capsules, or extended-release tablets for adults, the therapeutic goal remains the same: stabilizing the brain’s electrical and chemical environment.
However, treatment requires medical supervision, as periodic monitoring of liver function, platelet counts, and serum drug levels may be recommended to ensure safety and effectiveness.
Valproate pronunciation is typically val-pro-ate. Whether it is administered as valproate syrup for pediatric patients or extended-release tablets for adults, the goal remains the same: stabilizing the electrical and chemical environment of the brain.
How Valproate Works
When patients ask, “What does valproate do to the brain?” I like to use the analogy of a “volume knob.” In conditions like epilepsy or mania, certain brain circuits are “turned up” too high, firing rapidly and uncontrollably. Valproate helps turn that volume back down to a manageable level.
The GABA Connection
The primary valproate MOA (mechanism of action) involves a neurotransmitter called gamma-aminobutyric acid, or GABA. GABA is the brain’s primary inhibitory neurotransmitter—essentially the “brakes” of the central nervous system. Valproate works by:
- Increasing the production and release of GABA.
- Inhibiting the enzymes that break GABA down.
By strengthening the GABA system, valproate helps the brain stay in a “calm” state, preventing the rapid-fire electrical storms of a seizure or the runaway thoughts of a manic episode.
Ion Channel Modulation
Beyond GABA, valproate also influences the way sodium and calcium ions move in and out of brain cells. Blocking certain voltage-gated sodium channels prevents neurons from firing at pathologically high frequencies.
This dual action—strengthening the “brakes” while quieting the “engine”—is why it is such an effective broad-spectrum stabilizer.
Dosage and Administration
Finding the correct valproate dosage is a highly individualized process. Unlike many medications where a “standard” dose fits most adults, valproate requires a strategy called “therapeutic drug monitoring” (TDM).
The Importance of Blood Levels
In my clinical experience, I’ve found that two patients taking the exact same milligram dose can have vastly different amounts of the drug in their bloodstream. This is because our livers process valproate at different speeds.
- Typical Range: For most psychiatric or neurological conditions, the “sweet spot” in the blood is between 50 and 100 µg/mL (micrograms per milliliter), though some patients require up to 125 µg/mL for acute mania.
- Monitoring: Your doctor will order blood tests—usually taken in the morning before your first dose—to ensure you are in the therapeutic window and to monitor liver function and platelet counts.
Formulations and Timing
The way you take valproate matters.
- Delayed-Release vs. Extended-Release: Most modern prescriptions use divalproex sodium (Depakote ER) to minimize gastrointestinal distress.
- The 20 mg Nuance: While doses are usually in the 250 mg to 500 mg range, very small adjustments (like a 20 mg valproate equivalent shift in some liquid or specialized pediatric form) can sometimes be the difference between a side effect being tolerable or overwhelming.
A nuance I often observe is the interplay between valproate and a patient’s circadian rhythm. Because valproate can be sedating, the timing of the dose is vital.
The Nuance: I once worked with a patient who felt “foggy” every morning. We discovered that by moving her largest dose to 8:00 PM, we weren’t just helping her sleep—we were aligning the medication’s peak with her brain’s natural wind-down period.
This allowed her executive function to remain sharp during work hours. Good sleep hygiene isn’t just a lifestyle choice; it provides the biological “scaffolding” that allows valproate to do its job effectively.
Side Effects and Management
While valproate is an effective stabilizer, it is not without a physical “price tag.” In my sessions, we focus heavily on experience integration—learning how to live with the medication without losing quality of life.
Common Side Effects
| Side Effect | Frequency | Management Strategy |
| Weight Gain | Very Common | Focus on a low-glycemic diet; monitor insulin resistance. |
| Hair Loss/Thinning | Common | Usually temporary; supplementation with zinc or selenium (with MD approval). |
| Hand Tremor | Moderate | Often dose-dependent; avoiding excessive caffeine can help. |
| Nausea/GI Upset | Common | Taking it with food or using divalproex (delayed-release) forms. |
The Challenges of Weight and Hair
Two of the most distressing questions I get are, “Does sodium valproate cause hair loss?” and “How do I reduce weight gain due to sodium valproate?”
These concerns are common and valid, because while sodium valproate can be highly effective, metabolic and cosmetic side effects can affect adherence and quality of life. The good news is that both issues are often manageable with the right strategy.
1. Hair Loss (Thinning)
This is usually a form of telogen effluvium, a temporary shift of hair follicles into the shedding phase rather than permanent follicle damage.
It most commonly appears 3–6 months after starting treatment or after a dose increase. Hair may seem thinner overall, with increased shedding during washing or brushing.
In many cases, the hair regrows once the body adapts, the dose stabilizes, or the medication is adjusted by a clinician. Sometimes texture changes can also occur, such as curlier or finer hair.
Helpful strategies may include:
- Ensuring adequate protein intake, since hair is protein-based tissue.
- Checking for iron deficiency, thyroid issues, vitamin D deficiency, or zinc deficiency, which can worsen shedding.
- Avoiding harsh chemical treatments or excessive heat styling during active shedding.
- Discussing dose timing or alternative medications with a doctor if shedding is severe.
- Some clinicians may recommend supplements such as biotin or zinc, but only after medical review.
2. Weight Gain
Valproate can increase appetite, alter insulin sensitivity, and in some people reduce energy expenditure, making weight gain more likely over time.
This can be gradual and may be more noticeable in the first several months of therapy. Not everyone gains weight, but those who do often notice stronger cravings or increased hunger.
I encourage patients to view this through the lens of adaptation: we are changing brain signaling, and the body may respond metabolically. That means lifestyle support should be considered part of treatment, not an afterthought.
Helpful strategies may include:
- Regular moderate exercise (walking, resistance training, cycling, swimming).
- Prioritizing protein and fiber-rich meals to improve fullness.
- Reducing liquid calories and ultra-processed snacks.
- Maintaining good hydration, which can help with appetite control.
- Tracking weight weekly rather than obsessing daily.
- Protecting sleep, since poor sleep can worsen hunger hormones.
- Asking a doctor whether the dose, timing, or alternative medications are appropriate if weight gain is substantial.
Important Monitoring Considerations
Because sodium valproate can also affect liver enzymes and metabolic markers, clinicians may periodically monitor:
- Weight / BMI / waist circumference
- Liver function tests
- Blood sugar or lipids when relevant
- Overall medication effectiveness vs side effects
Reassurance
Hair thinning from valproate is usually reversible, and weight gain is often manageable with early intervention. The key is not to stop the medication abruptly, especially if it is controlling seizures or stabilizing mood. Instead, work with your clinician to balance benefits, side effects, and long-term health.
Serious Risks
While rare, we must monitor for:
- Hepatotoxicity: Liver inflammation, most common in the first six months.
- Pancreatitis: Severe abdominal pain requires immediate ER attention.
Special Risks and Contraindications
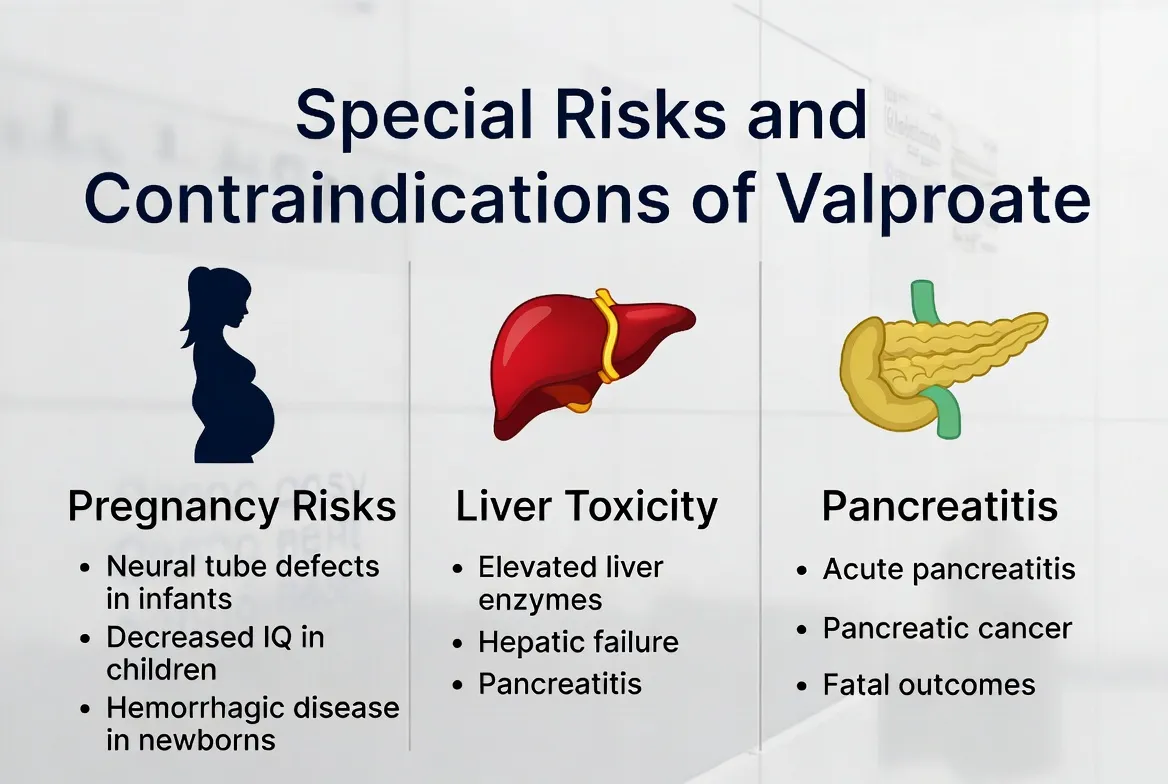
In my practice, the conversation around valproate shifts significantly when discussing specific populations. Because valproate is a systemic medication—affecting the liver, hormones, and even fetal development—there are several “red flag” areas where clinical caution is not just recommended, but mandatory.
Pregnancy and Teratogenicity
The most critical safety concern is whether valproate is safe in pregnancy. The answer, backed by decades of data, is generally no.
Valproate carries a high risk of major congenital malformations, particularly neural tube defects like spina bifida, and has been linked to lower IQ and developmental delays in children exposed in utero.
The Nuance: For women of childbearing age, I emphasize a “prevention-first” strategy. This involves:
- Using highly effective contraception.
- Taking high-dose folic acid (if pregnancy is a possibility).
- Engaging in “preconception counseling” to transition to safer mood stabilizers like lamotrigine before attempting to conceive.
Polycystic Ovary Syndrome (PCOS) Risk
The most critical safety concern is whether valproate is safe in pregnancy. The answer, backed by decades of data, is generally no.
Valproate carries a high risk of major congenital malformations, particularly neural tube defects such as spina bifida, and has also been linked to lower IQ, language delay, and developmental difficulties in children exposed in utero.
Risk may be higher at larger doses and during the first trimester, when early fetal organs are forming.
The Nuance: For women of childbearing age, I emphasize a prevention-first strategy. This involves:
- Using highly effective contraception while taking valproate.
- Taking high-dose folic acid if pregnancy is a possibility, ideally before conception.
- Engaging in preconception counseling to transition to safer mood stabilizers such as lamotrigine before attempting to conceive.
- Reviewing all medications regularly with a clinician to minimize unnecessary risks.
- Never stopping valproate abruptly without medical supervision, as seizure relapse or mood destabilization can also be dangerous during pregnancy.
Acute Porphyria
A rare but absolute contraindication is the risk of valproate use in patients with porphyria. Porphyrias are a group of rare inherited metabolic disorders that disrupt the body’s production of heme, an essential component of hemoglobin and many enzymes.
Because valproate is considered porphyrinogenic—meaning it can increase the buildup of toxic heme precursors—it is generally unsafe in individuals with acute hepatic porphyrias.
Using valproate in these patients can precipitate severe attacks marked by intense abdominal pain, vomiting, rapid heart rate, neuropathy, psychiatric symptoms, and potentially life-threatening neurological crises such as seizures, paralysis, or respiratory failure.
For this reason, a known history of acute porphyria should always be discussed before prescribing valproate, and safer alternative medications are typically preferred.
Drug Interactions and Monitoring
Valproate is what we call a “social” drug—it likes to interact with almost everything else in the medicine cabinet. Understanding valproate interactions is vital for avoiding accidental toxicity.
Common Interactions
- Other Anticonvulsants: Taking valproate with lamotrigine can double the levels of lamotrigine in your blood, increasing the risk of a serious rash (Stevens-Johnson syndrome).
- Aspirin can displace valproate from protein binding sites, leading to higher “free” levels and potential toxicity.
- Anticoagulants: Valproate can thin the blood (affecting platelets), so it must be used cautiously with blood thinners like warfarin.
How long does valproate stay in your system?
The typical half-life is 9 to 16 hours. This means that within about two to three days of stopping the medication, it is mostly cleared from the bloodstream. However, the effects on brain chemistry and neuroplasticity can linger for weeks, which is why we never stop this medication “cold turkey.”
In my experience, consistency is key. I advise patients to try to stay with the same manufacturer for their refills, as slight differences in how the “fillers” in a pill dissolve can occasionally cause minor fluctuations in blood levels.
Frequently Asked Questions
Is valproate the same as Depakote?
Yes, Depakote is simply a specific valproate brand name. It contains divalproex sodium, which the body converts into the active valproate ion once digested.
How does valproate work for mental health?
It acts as a chemical “stabilizer” by increasing GABA (the brain’s calming chemical) and quieting overactive electrical signals that lead to mania or mood swings.
Can valproate cause hair loss or weight gain?
Yes. These are the two most common “lifestyle” side effects. Hair thinning is often temporary, while weight gain usually requires active nutritional management and portion control.
Is valproate safe during pregnancy?
No. It is one of the highest-risk medications for birth defects. It should only be used in women of childbearing age if no other treatment is effective and strict birth control is in place.
Can patients with porphyria take valproate?
No. Valproate is contraindicated in acute porphyria because it can trigger a severe, dangerous metabolic crisis.
Conclusion
Valproate remains one of the most powerful tools in our neurological and psychiatric arsenal. Whether it is quieting the “electrical storms” of epilepsy or providing a firm “floor” for someone struggling with the highs and lows of bipolar disorder, its efficacy is undeniable.
However, the secret to success with valproate isn’t just taking the pill—it’s the monitoring and management.
By staying on top of blood tests, being proactive about metabolic health, and maintaining an open dialogue with your healthcare team about side effects, you can harness the benefits of this medication while protecting your overall quality of life.
You are the expert on your own body; use that expertise to help your doctors fine-tune your treatment.
References & Resources
- National Institute of Mental Health (NIMH): Bipolar Disorder Medications
- Epilepsy Foundation: Valproic Acid Information
- American Journal of Psychiatry: Valproate and PCOS Risk Studies
- Bipolar Lives: Valproate (Depakote) Guide
Related Posts






Subscribe to Our Newsletter
Get mental health tips, updates, and resources delivered to your inbox.
MORE from Author
Read More In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure…
In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure… We all have "up" days and "down" days. Perhaps you feel energized after a promotion or sluggish on a rainy…
We all have "up" days and "down" days. Perhaps you feel energized after a promotion or sluggish on a rainy…
 To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,…
To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,… To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…
To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…
Are you looking for a Therapist?
Connect with qualified mental health professionals who understand
bipolar disorder, mood changes, and emotional challenges.
Private • Supportive • Confidential