Bipolar Disorder Medications: Most Commonly Prescribed Drugs, Treatment Options & What Works Best

Medically reviewed by Carolina Estevez, Psy.D Updated Date: January 29, 2026

Living with bipolar disorder is often described as a journey through extremes. The highs of mania can feel like a surge of uncontrollable energy, while the lows of depression can feel like an immovable weight. Because this condition is fundamentally rooted in brain chemistry and biological rhythms, finding the right pharmacological intervention is critical.
In this comprehensive 2026 guide, we explore the landscape of bipolar disorder medications, detailing the most commonly prescribed drugs, how they work across different mood phases, and what the latest clinical research identifies as the most effective path toward long-term stability.
Understanding Medications for Bipolar Disorder
When discussing what medication is used for bipolar disorder, it is important to first establish that medication is the cornerstone of treatment. Unlike some mental health conditions where therapy alone might suffice for mild cases, bipolar disorder is a chronic biological condition that requires chemical stabilization to manage the neurotransmitters—such as dopamine, serotonin, and norepinephrine—that fluctuate during mood episodes.
The main treatments for bipolar disorder are designed to serve two distinct purposes:
- Acute Treatment: Bringing a person down from a manic peak or lifting them out of a depressive trough.
- Maintenance Treatment: Preventing future episodes and ensuring the person can live a functional, stable life between mood shifts.
While psychotherapy, sleep hygiene, and lifestyle changes are vital supportive pillars, common treatments for bipolar disorder almost always begin with a pharmacological foundation. Without this biological “floor” and “ceiling,” the emotional swings can become too severe for traditional coping mechanisms to take root.
What Is the Most Common Drug Used to Treat Bipolar Disorder?
If you were to look at the history of psychiatry, one name stands above the rest. When people ask, “What is the most common drug used to treat bipolar disorder?” the answer is frequently Lithium.
The Gold Standard: Lithium
Despite being one of the oldest medications in the psychiatric cabinet, lithium remains a first-line bipolar medication most commonly prescribed today. It is a naturally occurring salt that has a unique ability to stabilize mood from both ends—reducing the intensity of mania and significantly lowering the risk of depressive relapse and suicide.
Factors Influencing Frequency
However, the “most common” medication can vary based on:
- Geography: In some regions, atypical antipsychotics like Quetiapine have overtaken lithium in total prescriptions due to ease of use.
- Subtype: Those with Bipolar II may more frequently be prescribed anticonvulsants like Lamotrigine.
- Symptom Profile: If a patient presents with severe psychosis during mania, an antipsychotic is usually the immediate first choice over lithium.
Most Effective Treatment for Bipolar Disorder
If we look at the data from most effective treatment for bipolar disorder studies, the answer isn’t just a single pill; it’s a combination protocol.
Research consistently shows that patients who use a “cocktail” of a mood stabilizer (like Lithium) plus an atypical antipsychotic (like Vraylar) have a significantly lower relapse rate than those on monotherapy. Furthermore, the “biological” treatment must be paired with Psycheducation.
When a patient understands their “relapse signature”—the subtle changes in sleep or speech that happen before an episode—they can work with their doctor to adjust medication dosages in real-time, preventing a full-blown crisis.
1. Mood Stabilizers: The Foundation
Mood stabilizers are unique because they treat “from the top down” (mania) and “from the bottom up” (depression) without inducing the opposite pole.
- Lithium: Still the gold standard for suicide prevention and classic Bipolar I. It works by modulating neurotransmitters and neuroprotective factors, though it requires regular blood monitoring to prevent toxicity.
- Anticonvulsants: * Valproate (Depakote): Often more effective than Lithium for “mixed episodes” (simultaneous mania and depression).
- Lamotrigine (Lamictal): Primarily used for maintenance, specifically preventing the “crash” into depression, though it is less effective for acute mania.
2. Atypical Antipsychotics: The Rapid Responders
These medications act on dopamine and serotonin receptors. Because they work faster than mood stabilizers, they are often the first line of defense during a hospital admission.
- Metabolic Profile: While effective, they require monitoring for weight gain, cholesterol, and blood sugar changes.
- Versatility: Medications like Lurasidone (Latuda) and Cariprazine (Vraylar) are specifically FDA-approved for bipolar depression, a traditionally difficult-to-treat phase.
3. Antidepressants: The “Safety Net” Requirement
The primary danger of antidepressants in BD is mood destabilization.
- The Switch: Using an SSRI (like Fluoxetine) without a stabilizer can trigger a “manic switch” or “rapid cycling,” where the patient fluctuates between poles weekly or even daily.
- Combination Therapy: The most famous example is Symbyax, a pre-packaged combination of Fluoxetine (antidepressant) and Olanzapine (antipsychotic). The latter acts as a “ceiling,” preventing the antidepressant from pushing the mood too high.
4. Adjunctive Therapies: Symptom-Specific Support
These do not treat the underlying bipolar mechanism but manage the fallout of an episode.
- Sleep Architecture: Since sleep deprivation is a primary trigger for mania, using sedative-hypnotics or benzodiazepines (e.g., Lorazepam) can “reset” the biological clock during early signs of agitation.
- Limitations: Due to the risk of dependency and cognitive clouding, these are strictly short-term tools, usually tapered off once a primary stabilizer takes effect.
Comparison of Primary Bipolar Medication Classes
| Class | Primary Target | Key Benefit | Main Risk |
| Mood Stabilizers | Long-term stability | Reduces suicide risk; prevents relapse | Organ toxicity (Kidney/Thyroid) |
| Atypical Antipsychotics | Acute Mania / Depression | Rapid symptom control | Metabolic syndrome / Weight gain |
| Antidepressants | Severe Depressive “Lows” | Improves energy and outlook | Induction of Mania/Mixed states |
| Anti-Anxiety (Adjunct) | Agitation / Insomnia | Immediate calming effect | Dependency / Tolerance |
Lithium Medication for Bipolar Disorder

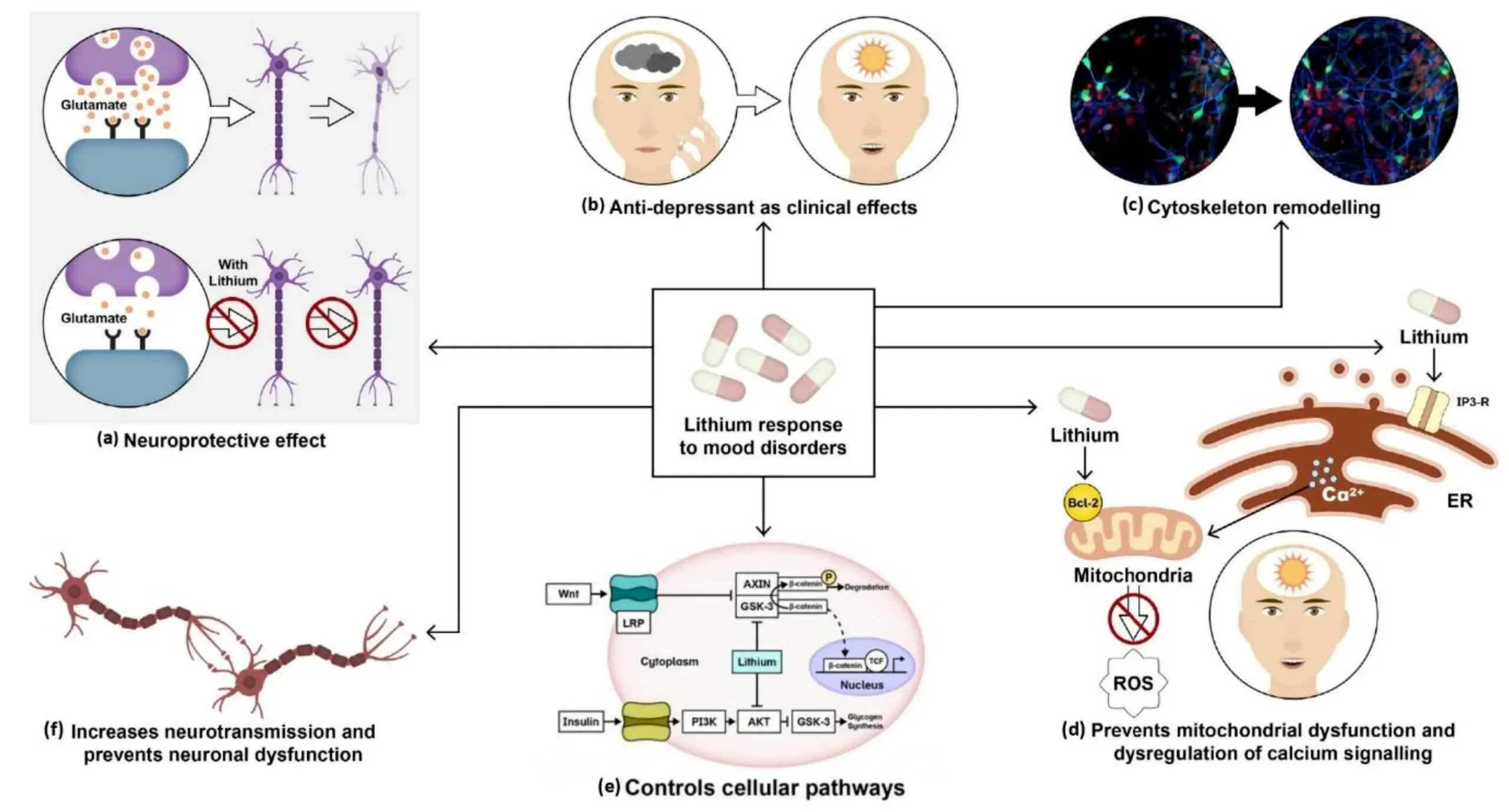
Because lithium medication for bipolar disorder is so foundational, it deserves a dedicated look. Lithium is unique because it is neuroprotective; it actually helps protect the brain’s neurons from the stress of mood cycles.
How It Works
Lithium influences the way sodium ions move through nerve and muscle cells. It also affects the “messaging” system within the brain, particularly involving glutamate.
The Maintenance Protocol
Lithium requires a high level of commitment:
- Blood Monitoring: Patients must undergo regular blood tests to ensure lithium levels stay within the “therapeutic window.” Too little is ineffective; too much can be toxic to the kidneys and thyroid.
- Hydration: Because it is a salt, staying hydrated is crucial for safety.
- Relapse Prevention: It is arguably the most effective medication at preventing hospitalization over a 10-year period.
Bipolar Medication Names List
For those seeking comprehensive bipolar medication names, the following tables categorize the most frequently used drugs in 2026 clinical practice.
Table 1: Mood Stabilizers (Anticonvulsants & Salts)
| Generic Name | Brand Name | Primary Target |
| Lithium Carbonate | Lithobid, Eskalith | Mania & Maintenance |
| Divalproex Sodium | Depakote | Acute Mania & Mixed States |
| Lamotrigine | Lamictal | Bipolar Depression |
| Carbamazepine | Tegretol | Mania (when others fail) |
Table 2: Atypical Antipsychotics
| Generic Name | Brand Name | Primary Target |
| Quetiapine | Seroquel | Mania & Depression |
| Aripiprazole | Abilify | Mania & Maintenance |
| Olanzapine | Zyprexa | Acute Mania |
| Lurasidone | Latuda | Bipolar Depression |
| Cariprazine | Vraylar | Mixed Episodes & Depression |
Table 3: Adjunct & Combination Medications
| Generic Name | Brand Name | Role |
|---|---|---|
| Fluoxetine/Olanzapine | Symbyax | Treatment-resistant Depression |
| Lorazepam | Ativan | Acute Agitation/Insomnia |
Bipolar 1 Medications List vs. Bipolar 2 Treatment
The choice of medication often hinges on whether the patient has Bipolar I or Bipolar II.
Bipolar 1 Medications List
In Bipolar I, the primary clinical danger is full-blown mania. Therefore, the bipolar 1 medications list focuses heavily on “capping the high.”
- First Choice: Lithium, Valproate, or Olanzapine.
- Psychosis Management: Intensive use of antipsychotics is common during acute phases.
Bipolar 2 Treatment Focus
In Bipolar II, the patient experiences hypomania (milder highs) but spends significantly more time in debilitating depression.
- Depression Focus: Lamotrigine is often the first-line choice because it is excellent for preventing “the drop.”
- Avoiding “The Switch”: Doctors are even more cautious with antidepressants in Bipolar II, as the risk of triggering hypomania or rapid cycling is high.
What Are the Top 10 Medications for Bipolar Disorder?
In 2026, the pharmacological landscape for bipolar disorder is defined by a “tiered” approach based on clinical efficacy and patient tolerability. Rather than a simple popularity contest, the top 10 medications for bipolar disorder are selected by clinicians for their ability to target specific phases of the illness (mania, depression, or maintenance).
- Lithium (Lithobid): The classic mood stabilizer and the only medication proven to significantly reduce suicide risk and provide long-term neuroprotection.
- Quetiapine (Seroquel): Unique for being one of the few drugs FDA-approved for both acute mania and bipolar depression.
- Lamotrigine (Lamictal): The preferred choice for Bipolar II, as it acts as a “buffer” against future depressive episodes.
- Divalproex (Depakote): Highly effective for acute mania and “mixed features”—where you feel both high energy and low mood simultaneously.
- Aripiprazole (Abilify): Often used for maintenance because it has fewer sedating side effects than other antipsychotics.
- Cariprazine (Vraylar): A modern powerhouse that treats the full spectrum of symptoms, from mania to the deepest depressive troughs.
- Lurasidone (Latuda): Specifically targeted at bipolar depression with a relatively low impact on weight and metabolic health.
- Olanzapine (Zyprexa): Frequently used in emergency settings to stop severe mania quickly due to its potent sedating and stabilizing effect.
- Lumateperone (Caplyta): A newer generation antipsychotic that modulates dopamine, serotonin, and glutamate, offering a “cleaner” side-effect profile.
- Risperidone (Risperdal/Uzedy): Available in both oral and newly approved extended-release injectable forms, making it a staple for ensuring long-term medication adherence.
Best Medication for Bipolar Depression and Anxiety

One of the most complex challenges in psychiatry is finding the best medication for bipolar depression and anxiety. Because traditional antidepressants can “trigger” mania, clinicians must look for medications that provide an “anti-anxiety” effect without causing a mood switch.
Treating the “Bipolar Low” Safely
Bipolar depression is fundamentally different from clinical (unipolar) depression. The best medication for bipolar depression and anxiety often involves:
- Quetiapine: Its metabolite, norquetiapine, has a direct effect on norepinephrine, which helps lift depression, while its sedating properties “quiet” anxiety.
- The “Antipsychotic-Antidepressant” Combo: Drugs like Symbyax (a combination of Olanzapine and Fluoxetine) are specifically designed to treat depression, while the antipsychotic acts as a safety guard against mania.
- Lamotrigine: While not a “rescue” drug for anxiety, it provides a stable foundation that reduces the frequency of the depressive crashes that often cause secondary anxiety.
Managing Co-occurring Anxiety
For many, anxiety isn’t just a symptom—it’s a constant companion. To treat this, doctors may add:
- Gabapentin: An anticonvulsant often used off-label for its calming effects.
- Buspirone: A non-habit-forming anti-anxiety medication that is safer for long-term use than benzodiazepines.
New Bipolar Medication List: What’s Changed Recently
As we move through 2026, the new bipolar medication list includes advancements that focus on convenience and metabolic safety.
- Extended-Release Injectables (UZEDY): In late 2025, the FDA approved new long-acting versions of risperidone that can be administered once a month or every two months. This is a game-changer for those who struggle with “pill fatigue.”
- Lumateperone (Caplyta) Expansion: Originally approved for schizophrenia, its 2025-2026 indications for both Bipolar I and II depression have made it a favorite for patients concerned about weight gain and diabetes risk.
- The Glutamate Frontier: While still in the final stages of research, new medications targeting the glutamate system (similar to how ketamine works) are emerging as rapid-acting options for treatment-resistant bipolar depression.
Typical Medications for Bipolar Disorder Across Mood Phases

Your medication plan is a living document. Typical medications for bipolar disorder shift depending on the “weather” of your mind:
- The Acute Manic Phase: Potent antipsychotics (Olanzapine, Risperidone) and “loading doses” of mood stabilizers (Valproate) are used to bring the person back to safety.
- The Acute Depressive Phase: Medications like Lurasidone or the Olanzapine-Fluoxetine combo are used to lift the mood without causing a “flip.”
- The Maintenance Phase: This is where the dose is lowered to the “minimum effective amount.” Lithium or Lamotrigine usually takes the lead here to keep the brain in a state of euthymia (a stable, balanced mood).
Mood Stabilizers (The Foundation)
Mood stabilizers are the cornerstone of long-term bipolar treatment. They help level out the “peaks” and “valleys” of the condition.
- Lithium (Lithobid): Historically, the gold standard and still a first-line treatment in 2026. It is highly effective for both mania and maintenance, and it is the only medication proven to significantly reduce suicide risk.
- Divalproex Sodium (Depakote): An anticonvulsant often used for acute mania and mixed episodes (feeling manic and depressed simultaneously).
- Lamotrigine (Lamictal): Primarily used for bipolar depression and maintenance. It is less effective for acute mania but excellent at preventing future depressive drops. Note: It requires a slow “titration” (dose increase) to avoid a rare but serious rash.
Atypical Antipsychotics (Second-Generation)
Modern antipsychotics are now frequently used as first-line agents, even without symptoms of psychosis, because they work quickly and effectively.
- Quetiapine (Seroquel): One of the few medications approved for all three phases: mania, depression, and maintenance.
- Cariprazine (Vraylar): Versatile for both mania and depression; it is often praised for its ability to treat the “mixed” symptoms of bipolar I.
- Lumateperone (Caplyta): A newer (FDA-approved 2021/2025) option specifically for bipolar I and II depression. In 2026, it is highly valued for having a lower risk of weight gain and metabolic side effects compared to older antipsychotics.
- Aripiprazole (Abilify): Common for maintenance and acute mania; often preferred for patients sensitive to sedation.
Latest 2025–2026 Approvals
The most recent medical developments have focused on “adherence”—helping patients stay on their meds more easily.
- UZEDY (Risperidone Extended-Release): Approved in late 2025 as a long-acting injectable (LAI). It provides maintenance treatment for Bipolar I through a subcutaneous injection once every one or two months, eliminating the need for daily pills.
- Subvenite: A newer formulation of lamotrigine (late 2025) designed to offer refined dosing and improved access for patients.
Bipolar Depression & The “Antidepressant Risk.”
Standard antidepressants (like Prozac or Lexapro) are rarely used alone in bipolar disorder because they can trigger a manic switch (pushing a patient into a high).
| Treatment Strategy | Preferred Medications |
| First-Line Monotherapy | Quetiapine, Lurasidone (Latuda), Lumateperone (Caplyta) |
| Combination Therapy | Symbyax (Olanzapine + Fluoxetine) |
| Adjunctive Therapy | Lurasidone added to Lithium or Valproate |
Essential Monitoring
Bipolar medications require active management.
- Lithium/Depakote: Requires regular blood tests to ensure the drug stays in the “therapeutic window” (high enough to work, low enough to avoid toxicity).
- Metabolic Checks: Antipsychotics can sometimes affect weight, blood sugar, and cholesterol, so annual physicals are critical.
Safety, Monitoring & Long-Term Medication Use

In 2026, the philosophy of bipolar care has shifted toward “Total Wellness Monitoring.” Taking medication is not just about checking a box; it is about managing your systemic health to ensure your body remains a healthy environment for your brain.
Blood Tests and Health Monitoring
Because medications like Lithium and Valproate have a narrow “therapeutic window,” regular blood tests are mandatory.
- Lithium Levels: Typically checked every 3–6 months once stable to prevent toxicity.
- Kidney and Thyroid Function: Lithium can affect the kidneys (eGFR) and thyroid (TSH), requiring biannual checks.
- Liver Function (LFTs): Essential for those on Valproate or Carbamazepine.
- Metabolic Monitoring: For those on atypical antipsychotics, doctors monitor weight, blood sugar (HbA1c), and lipid profiles to prevent metabolic syndrome.
The Importance of Adherence
“Pill fatigue” is real, but the danger of stopping medication abruptly is great. Rapid discontinuation is the 1 trigger for a rebound manic episode, which can be more severe than the original symptoms. Modern 2026 options, like the newly expanded UZEDY (risperidone extended-release), allow for once-monthly or even once-every-two-months injections, significantly reducing the burden of daily adherence.
Frequently Asked Questions
What medication is used for bipolar disorder?
Bipolar disorder is primarily managed with mood stabilizers (like Lithium and Lamotrigine), atypical antipsychotics (like Quetiapine and Vraylar), and occasionally anticonvulsants (like Divalproex). These are often used in combination to address both the “highs” and “lows” of the condition.
What is the most common drug used to treat bipolar disorder?
Lithium remains the most historically significant and common first-line treatment for Bipolar I. However, atypical antipsychotics like Quetiapine and Aripiprazole have become equally common in 2026 due to their broad efficacy across both manic and depressive phases.
What are the top 10 medications for bipolar disorder?
The current top 10 list includes: Lithium, Quetiapine, Lamotrigine, Divalproex, Aripiprazole, Cariprazine (Vraylar), Lurasidone (Latuda), Olanzapine, Lumateperone (Caplyta), and Risperidone (Uzedy). Each is selected based on the patient’s specific symptoms and bipolar subtype.
What is the best medication for bipolar disorder and anxiety?
Medications like Quetiapine and Lurasidone are often effective because they stabilize mood while providing sedative or anti-anxiety properties. Adjuncts like Gabapentin or Buspirone may also be prescribed specifically to target anxiety without the risks associated with standard antidepressants.
Is lithium still used for bipolar disorder in 2026?
Yes, Lithium is still the “gold standard” for preventing suicide and managing classic Bipolar I mania. While newer drugs offer more metabolism-friendly profiles, Lithium’s neuroprotective benefits and efficacy in preventing relapse keep it at the forefront of clinical practice.
Conclusion
Finding the perfect medication plan for bipolar disorder is rarely a one-step process. It is a collaborative effort between you and your healthcare provider—a dance of fine-tuning dosages and balancing side effects against stability.
Whether you are starting with a foundation of lithium medication for bipolar or exploring the latest atypical antipsychotics on the new bipolar medication list, the goal remains the same: euthymia. Stability is not just the absence of an episode; it is the presence of a clear, functional life. With the right bipolar medication names in your toolkit and a commitment to long-term monitoring, the “rollercoaster” of bipolar disorder can finally be brought to a halt.
Authoritative References
1. National Institute of Mental Health (NIMH)
2. American Psychiatric Association (APA)
3. CANMAT and ISBD Guidelines (2023–2026 Update)
4. National Institute for Health and Care Excellence (NICE)
5. Mayo Clinic: Bipolar Diagnosis & Treatment
Related Posts





Subscribe to Our Newsletter
Get mental health tips, updates, and resources delivered to your inbox.
MORE from Author
Read More In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure…
In my practice as a clinical psychologist, I often observe that the difference between a patient who crumbles under pressure… We all have "up" days and "down" days. Perhaps you feel energized after a promotion or sluggish on a rainy…
We all have "up" days and "down" days. Perhaps you feel energized after a promotion or sluggish on a rainy…
 To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,…
To define bipolar disorder accurately, we must look at it as a chronic mood dysregulation condition. In psychology and medicine,… To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…
To answer whether bipolar fits the bill, we first have to define what a neurodivergent person actually is. The term…
Are you looking for a Therapist?
Connect with qualified mental health professionals who understand
bipolar disorder, mood changes, and emotional challenges.
Private • Supportive • Confidential